ChooseLife : It is clear to me, that those on higher sugars are more prone to mental health disorders – Sugar intake – Whitehall Study/ Therefore, it is almost certain, that those needing antidepressants, will be more likely to also be closer to diabetes/sugar dis-regulation, than those on lower simple sugar diets, higher magnesium/greens/Omega3 et al.
Oxygen and sugar share the same space in blood, hence, when that blood is also being shared with a growing baby, as is the focus below, it is no wonder that struggle for space may become more fragile and a narrower range can be tolerated.
” Gestational diabetes, a type of diabetes that can develop during pregnancy in women, can increase the risk of certain complications for both the mother and baby, including risks of high blood pressure for the expectant mother, needing a cesarean section delivery, having low blood sugar for the baby and developing type 2 diabetes later in life for the baby.
After analyzing that data and taking a close look at antidepressant exposure, the researchers found that specifically venlafaxine and amitriptyline were associated with a 27% and 52% increased risk of gestational diabetes.
While the risk was greatest for those two antidepressants, the researchers also found that gestational diabetes risk increased with the longer any antidepressant was taken.”
ChooseLife : If only these people of science were allowed to put 2 and 2 together. The use of Antidepressants is almost certainly a sign of longer term sugar problems, which turn everyday struggles into unbearable burdens, to unfortunate individuals with less robust Liver and/or Pancreatic function. Prolonged Low Blood Sugar/Hypoglycemia is a precursive condition to Diabetes, known to cause Mental Health dysfunction.
The spleen is my favourite organ in the body. As an acupuncturist, I am not
really supposed to play favourites, saying you love one organ more than the
others is like a parent declaring that they love one of their children more,
but I feel like I have a special connection with the spleen. I talk about it a
lot and I seem to write about it even more. It is a hard working and often
under appreciated little organ, so it is my duty, and my privilege to give it
some much needed love and attention.
The spleen is an organ that doesn’t really get discussed very much in relation to the other organs of the body. I think its role in Western medicine is perhaps seen as less ‘vital’ than the other organs, but the role of the spleen in Western medicine is very different than its role in Chinese medicine.
The Spleen In Western Medicine
In Western medicine the spleen is part of the immune system and the largest organ in the lymphatic system. It is where red blood cells are recycled and where white blood cells, called lymphocytes, are stored. It is possible to live without a spleen. You can lacerate or rupture your spleen in a car accident or playing contact sports (or via any severe physical trauma) and the spleen may have to be repaired or removed completely (called a splenectomy). Although it is possible to live without a spleen because other organs overcompensate and take over many of its important functions, it makes a person more susceptible to infections and ultimately compromises their immune system.
The Spleen In Chinese Medicine
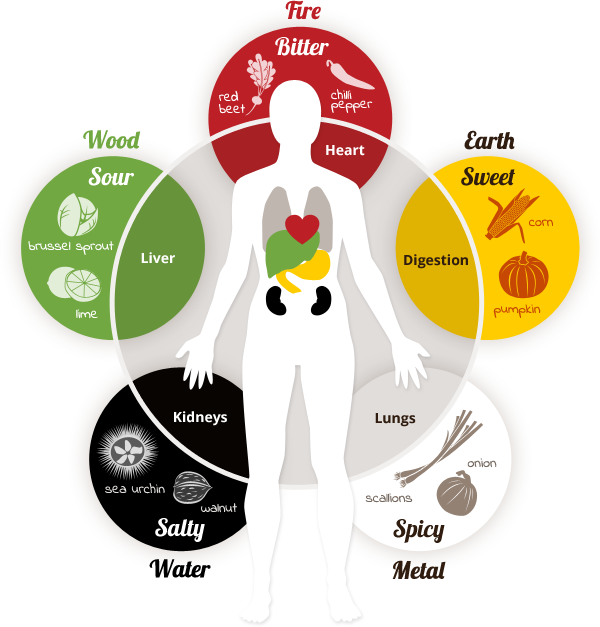
This lovely image is from thespicedoc.com and designed by Patricia Callison
The spleen has a fundamental role in Chinese medicine. It, paired with the stomach, are the main organs of digestion and are responsible for digestion and distribution of food and nutrients throughout the body. The spleen extracts qi from the food we eat that is used by the body to build immunity (wei qi), keep things moving freely (stagnation leads to disease), the proper functioning of the other organs and helps to regulate mental functions and emotions.
Why Our Culture Is Hard On The Spleen
It is very common in our culture to have a deficiency of the spleen. Because the spleen is the main organ of not only digestion, but processing, it is responsible for processing the food and drink that we consume, as well as all of the stimulus that comes in through our sense organs. We are a culture that values doing many things at once. The more productive we can be, the more we are praised at our jobs and in life. This philosophy is contrary to the health of the spleen. In Chinese medicine, to keep the spleen healthy, it is important to do one thing at a time, and as mindfully as possible. The idea is that the spleen is then able to use all of its energies to process one thing, rather than having to process many things at once, which wipes out its energy stores, or spleen qi. Examples of doing many things at once are eating (taking in food/drink) while watching TV (taking in stimulus). Or eating while sitting at your computer working. These are commonplace in a culture where everyone has too much to do and is always short on time. This is one of the biggest reasons that so many people suffer with a deficiency of their spleen qi. So, do one thing at a time. If you are going to eat, just eat. Really concentrate and be mindful about what you are doing. Enjoy and savour your food, this will not only help your spleen, but lead you to be more relaxed and help you digest more efficiently too.
A Strong And Balanced Spleen
People with strong and balanced spleen energy have the following
characteristics:
responsible
practical
hard working
strong
like to nurture themselves and others
active
stable
excellent endurance
good appetites
good, healthy digestions
strong limbs
are orderly and careful
often very creative
have fertile imaginations
A Spleen Imbalance
People with an imbalance of their spleen often display the following
characteristics:
chronically tired
a feeling of being “stuck”
in their lives
physical and/or mental
stagnation
weak digestion (lots of
digestive issues)
poor appetite
diminished sense of taste
loose stools
abdominal bloating and
tenderness
masses in the abdomen
weight problems (either
overweight without overeating or underweight without the ability to gain)
Spleen Qi Deficiency
A deficiency of spleen qi can be caused by many things. Eating a poor diet
of mostly refined, highly processed foods where the body is not receiving
enough nourishment is certainly common, especially in industrialized nations
where foods tend to be overly processed and many people make poor food choices.
Another cause is simply our hectic lifestyles. As I mentioned above, we are a
culture of multitasking, and this is particularly hard on the tiny organ that
is responsible for doing all the processing. If it is constantly overloaded,
then it will become exhausted, leading to spleen qi deficiency. Another cause,
and this is also extremely common, is the emotional aspect of the spleen. In
Chinese medicine, every organ is associated with an emotion. An excess of that
emotion can damage the related organ, and likewise, when the organ is out of
balance, it can have a strong effect on the corresponding emotion. The emotion
of the spleen in worry/over thinking. If there is one emotion that I see more
than any other in clinic, it is WORRY. An excess of worry and over thinking, as
well as having a hard time just shutting off your brain, is damaging to the
spleen. And we do that so much in our society. The pressures on us are
enormous, and people are simply overworked and overstressed. So, poor
nutrition, multitasking and a propensity to worry are all part of our culture,
and all are affecting our poor, overworked spleens. It’s no wonder spleen qi
deficiency is so common.
Here are some symptoms of spleen qi deficiency so you know what to look for:
weakness of the whole body
fatigue
loose stools with
undigested food
a pale tongue with a thin
white coat and teeth marks on the sides
a weak pulse
weakness of the arms and
legs
weak muscles
prolapse of organs (such as
hemorrhoids, uterus, bladder, intestines)
The symptoms above all point to a spleen imbalance. There is good news though. There is wonderful nutritional therapy for deficient spleen qi, and as many Chinese doctors have known for centuries, food is the best medicine.
The Thermal Nature Of Foods In Chinese Medicine
When we talk about nutritional therapy in Chinese medicine, which is an important modality, we talk about the thermal nature of foods. This can be a bit of a difficult concept to understand at first, but once it’s explained, it actually starts to make a lot of sense. Thermal nature is not just how physically cold or hot a food is as a result of cooking. In Chinese medicine, all foods are seen to have a fundamentally thermal nature, either warming, cooling or neutral, and these are important to know as they have a direct effect on the body. In the context of Chinese medicine it is also important to know the thermal nature of your body, which is measured by the relative yin and yang energies it encompasses. For example, if a person comes to you with a red face, bloodshot eyes, outbursts of anger and is shouting, it is pretty safe to determine that that person has an excess of yang energy and thus, should eat cooling foods and stay away from warming ones until the balance of yin and yang is reestablished. Every organ also, has a temperature that it prefers, so it is good to know all these things when thinking about food therapy in terms of health and disease.
Food Therapy For Spleen Qi Deficiency
With foods thermal nature in mind, the spleen likes to be warm and dry. So
if you have spleen qi deficiency, you want to eat foods that are warming, or at
least neutral to help build the spleens energy. Cold foods should be avoided as
they weaken digestion. Also, foods that are cold in temperature take more
energy for the spleen to digest and are seen to extinguish the digestive fire.
The flavour associated with the spleen is sweet, so as a rule, sweet foods are
prescribed to correct a deficiency.
One of the best foods to build spleen qi is cooked white rice, often eaten in the form of congee or jook. Congee is essentially a porridge made of overcooked rice and water. You may add other ingredients depending on your condition and taste. For spleen qi deficiency or any weakness of the spleen, warming ingredients would be appropriate. See the list below.
Beneficial Spleen Foods
Vegetables
pumpkin
yam
black beans
garbanzo beans
carrot
parsnip
squash
peas
sweet potato
onion
leek
Spices
black pepper
ginger
nutmeg
cinnamon
fennel
garlic
Sweeteners (in small amounts)
barley malt
rice syrup
molasses
cherries
dates
Animal Products (if the deficiency is severe)
mackerel
tuna
halibut
anchovy
beef
beef liver or kidney
turkey
chicken
lamb
butter
Chewing foods well is also important when spleen energy is weak. This helps to break down foods before they get to the spleen and means the spleen has less work to do and conserve its energy. Eating things like soups are beneficial because they are cooked until soft and are less work for the spleen to digest. And finally, the preparation of food is also a factor in helping to build up spleen qi. Eating on the run and eating out mean that you are not taking the time and intention to mindfully prepare the foods that you are eating. To prepare foods with care infuses them with healing energies that the whole body, and especially the spleen, needs. So take the time to prepare the foods that you are eating with love, your spleen will appreciate it. 🙂
Abstract Intake of sweet food, beverages and added sugars has been linked with depressive symptoms in several populations. Aim of this study was to investigate systematically cross-sectional and prospective associations between sweet food/beverage intake, common mental disorder (CMD) and depression and to examine the role of reverse causation (influence of mood on intake) as potential explanation for the observed linkage. We analysed repeated measures (23,245 person-observations) from the Whitehall II study using random effects regression.
Diet was assessed using food frequency questionnaires, mood using validated questionnaires. Cross-sectional analyses showed positive associations.
In prospective analyses, men in the highest tertile of sugar intake from sweet food/beverages had a 23% increased odds of incident CMD after 5 years (95% CI: 1.02, 1.48) independent of health behaviours, socio-demographic and diet-related factors, adiposity and other diseases.
The odds of recurrent depression were increased in the highest tertile for both sexes, but not statistically significant when diet-related factors were included in the model (OR 1.47; 95% CI: 0.98, 2.22). Neither CMD nor depression predicted intake changes.
Our research confirms an adverse effect of sugar intake from sweet food/beverage on long-term psychological health and suggests that lower intake of sugar may be associated with better psychological health.
ChooseLife : This is the beginning post in a research stream I will undertake, to demonstrate the multi faceted path of destruction simple sugars may wreak, on susceptible individuals mental and physical health. Many years ago I read Moreless responding to a question on the general cause of Depression, just four words, which at the time did not click for me, but does now “prolonged low blood sugar“, the thought streams back to Carey Reams exceptional interview on Blood Sugars available here = Dr Carey Reams Interview on Hypoglycemia
Aluminium salts are common adjuvants in vaccines given to children. Their physical, chemical and biological properties have recently been reviewed [1]. However, a debate continues as to whether neonate and infant exposure to aluminium through vaccination is biologically significant with respect to their exposure to aluminium through other routes and especially diet. For example, paediatricians, responsible for administering the vaccine schedule for children, seem in particular, to be uninformed about the properties of aluminium adjuvants and their mode of action in vaccines. This apparent ignorance of the published scientific literature is unexpected in those charged with the wellbeing of neonates and infants and especially in the light of Janeway’s description of alum adjuvant as ‘the immunologist’s dirty little secret’ [2]. Paediatricians such as recently (07/04/2019) Andrew Pollard in The Sunday Times, have a habit of reverting to pure ‘baby talk’ when for example; describing how much aluminium is present in an infant vaccine. They use terms such as ‘minuscule’ and ‘teeny-weeny’ to tell anyone, who asks, how little aluminium there is in a vaccine. They usually then proceed to compare the amount of aluminium in a vaccine with the amount of aluminium in (an adult’s) diet. There are, of course, more accurate, understandable ways to inform parents and other interested parties how much aluminium is present in a vaccine, and I shall endeavour to achieve this herein. An appreciation of how much aluminium is present in a single injection of a vaccine is critical to understanding how aluminium adjuvants are effective in stimulating the immune response.
2. How much aluminium is found in vaccines?
Currently about 20 childhood vaccines include an aluminium adjuvant. Vaccine industry literature (for example; https://www.medicines.org.uk/emc/product/2586/smpc) expresses the aluminium content of an individual vaccine as an amount (weight) of aluminium (not aluminium salt) per unit volume of a vaccine (usually 0.5 mL). Industry does this to account for the fact that there are no strict molecular weights for the polymeric aluminium salts that are used as adjuvants in vaccinations. They prepare acid digests of the adjuvants and measure their total aluminium using ICP MS. This is not explained in the literature they provide with vaccines and can cause confusion for some as the actual weight of hydrated aluminium salt (e.g. aluminium oxyhydroxide, aluminium hydroxyphosphate and aluminium hydroxyphosphatesulphate) in any vaccine preparation is actually approximately ten fold higher. The aluminium salt is the major component of a vaccine (after water) and its high content is why vaccine preparations are invariably cloudy in appearance [1]. As an example, GlaxoSmithKline’s Infanrix Hexa vaccine is reported by the manufacturer to contain 0.82 mg of aluminium per vaccine (0.5 mL). Thus, the weight of aluminium salt in this vaccine is approximately 8 mg, which is approximately ten times the weight of all of the other components of the vaccine when combined. An aluminium-adjuvanted vaccine is essentially a very high concentration of an aluminium salt (8 mg/0.5 mL or 16 mg/mL or 16 g/L) in which just μg of other vaccine components including antigens and other excipients are occluded.
3. Is the amount of aluminium in a vaccine ‘minuscule’?
Generally, in the United Kingdom the first dose of Infanrix Hexa vaccine is injected into muscle when an infant is 8 weeks old. All 8 mg of the aluminium salt (or 0.82 mg of aluminium) will immediately be systemic; it is inside the infant’s body. The repercussions of this being that the injected aluminium may only leave the body through its excretion in either the infant’s urine or sweat. What is the immediate biological response to this exposure to aluminium adjuvant? Aluminium is described as a silent visitor to the human body. What this means is that in the evolution of life on Earth and latterly human evolution, no historic signature is found as evidence for previous exposure to aluminium [3]. By way of comparison with another toxic and non-essential metal, if the adjuvant used in a vaccine was composed of a cadmium salt its injection would immediately initiate a counter-response by the body in an attempt to remove the toxicant. Proteins known to bind and help in the detoxification of cadmium are produced and this is a sure sign that biochemistry had previously encountered non-essential cadmium and selected it out of essential biochemical pathways. Such restorative attempts at detoxification are not triggered for biologically available aluminium and so the ‘processing’ of aluminium adjuvant at the injection site of a vaccine is completely adventitious and one might suggest, random and chaotic. The latter because the fate of aluminium in the body, unlike essential and other non-essential metals, is not subject to any form of homeostasis. Myriad chemical and biological processes will initiate the slow redistribution of the injected aluminium throughout the infant’s body. These steps will involve the processes of disaggregation, dissolution, complexation, precipitation, distribution, cellular uptake and translocation. The description of each one of these processes is an essay in itself and we have addressed them all in many complementary publications [1]. An important and vaccination-specific distinction to make at this point and to carry forward to the following discussion is that aluminium injected into muscle as an adjuvant in a vaccine potentially has uninterrupted access to the infant brain. This is because there is no prerequisite for its passage via the liver, the most prominent organ of detoxification in humans.
We asked if 0.82 mg of systemically available aluminium administered as a single dose in a vaccine is, as some paediatricians would suggest, a minuscule amount of aluminium, for example, as compared to aluminium in the diet. Infants receiving Infanrix Hexa vaccine at 8 weeks of age are concurrently either being breast or formula fed. Data show that the former is likely to result in an 8 week old infant ingesting up to 0.1 mg of aluminium each day [4,5]. On the day an infant receives 8 mg of an aluminium salt, or 0.82 mg of aluminium, in a vaccine it will also ingest 0.1 mg of aluminium in breast milk. However, what proportion of this 0.1 mg of dietary aluminium will be absorbed across the infant gut? Previous research has asked a similar question [6]. The reality is that data for the absorption of aluminium across the infant gut do not presently exist and one has to apply gastrointestinal absorption data obtained for adults. The oft-cited value for adults is that less than 0.1% of ingested aluminium in diet is actually absorbed [7]. The infant gut at 8 weeks is incomplete [8] and is likely to be much more permeable to dietary aluminium, perhaps as much as 100 times more permeable. Applying such clearly conditional criteria it can be estimated that 10% of ingested aluminium or 0.01 mg/day of aluminium in breast milk is absorbed across the infant gastrointestinal tract. However, the blood carrying nutrients and toxins that have been absorbed from the gut, to the rest of the body must first pass through the liver, the major detoxification system of the body. Data on the efficiency of the liver in removing aluminium from the blood is, at best, incomplete in adults [9] and completely unknown in infants. If it is estimated that the liver is 75% efficient in this respect for adults then it is probably only 50% efficient in an infant. When these various conditional factors are accounted for it can be estimated that an infant’s exposure to systemically available aluminium from breast-feeding is approximately 0.005 mg of aluminium each day. In essence during the first 8 weeks or 56 days of life, breast-feeding ostensibly drip feeds an infant with a combined total of 0.28 mg of systemically available aluminium. On day 56 the infant receives a single dose of 0.82 mg of aluminium in the Infanrix Hexa vaccine, a dose equivalent to 3 times the amount of aluminium the infant received during the entire 55 days of life prior to its vaccination. It is well known, if highly unfortunate, that infant formulas are heavily contaminated with aluminium [10,11] and in a worst-case scenario an infant only being formula-fed from birth might be exposed to 0.030 mg of aluminium each day up to vaccination on day 56. Even in this worst-case scenario, the exposure to systemically available aluminium on vaccination day is 25 times higher through the vaccine than through the diet.
4. Acute versus chronic exposure to aluminium
Breast or formula feeding in an infant is a chronic exposure to aluminium. The infant is exposed to a small but continuous supply of systemically available aluminium, aluminium that has the potential to be stored in the infant’s body and excreted from the infant’s body in the urine. Perhaps, at no point during continuous chronic (drip feed) exposure in infancy (0–12 months of age) does the concentration of aluminium in any one physiological compartment increase to bring about overt toxicity. How does dietary exposure to aluminium in infants compare to exposure through vaccination, for example, a single Infanrix Hexa vaccine at 8 weeks of age? The concentration of aluminium (not aluminium salt) in an Infanrix Hexa vaccine upon its injection into muscle is, according to the manufacturer, 0.82 mg/0.5 mL or 1.64 mg/mL or 1.64 g/L or approximately 60 mmol/L. This is the concentration of total systemically available aluminium immediately present at the injection site of the vaccine and available to bring about biological effect. Aluminium adjuvants are not inert depots at the vaccine injection site; they are sources of biologically reactive aluminium [1]. This concentration of total aluminium at the injection site of a vaccine can be put into context by examining the cellular toxicity of aluminium [12] and specifically as identified in recent scientific publications. We can ask the question if we would expect this concentration of aluminium to produce biological effects including cell death at the vaccine injection site. A relevant cell to investigate are lymphocytes and research has demonstrated significant genotoxicity in lymphocytes exposed to only 0.020 mmol/L total aluminium [13]. Similarly, in another study using lymphocytes 0.6 mmol/L total aluminium resulted in significant immunosuppression in both T and B-lymphocytes [14]. Clearly, we would expect profound effects on lymphocytes at the injection site of a vaccine where the total aluminium concentration is 60 mmol/L. Macrophages, a characteristically robust cell, are susceptible to aluminium toxicity demonstrating 50% cell death at a total aluminium concentration of 10 mmol/L [15]. Other more sensitive cell lines would include neuroblastoma where cell viability is reduced by 50% by less than 1 mmol/L total aluminium [16] and similarly for primary hippocampal neurons exposed to only 0.05 mmol/L total aluminium [17]. The concentration of systemically available aluminium immediately present at the injection site of a vaccine is very high in comparison to studies on cell cytotoxicity in the scientific literature. It is an acute exposure to aluminium and it results in significant cytotoxicity including necrotic cell death [1]. The resulting tissue inflammation is the characteristic red mark on the skin at the injection point. This acute toxicity in the immediate vicinity of the injection site underlies the success of aluminium salts as adjuvants in vaccinations [1]. However, while some cells, both present at and infiltrating the injection site, are compromised and especially immediately, other cells act to remedy the situation by taking up aluminium adjuvant into their cytoplasm [18]. This action reduces the concentration of biologically reactive (toxic) aluminium at the injection site and locks away potentially cytotoxic aluminium in intracellular vesicles. Herein may be the real issue linking aluminium adjuvants and severe adverse events following a vaccine. These aluminium-loaded cells remain viable for days, potentially weeks, which means that they can transport their cargo of aluminium anywhere in the body including the infant brain. The recruitment of systemic cells including macrophages to the central nervous system is a widely documented phenomenon [19]. There is now a viable mechanism for the accelerated loading of an infant’s brain with aluminium and evidence to support such a mechanism was demonstrated in our recent paper on aluminium in brain tissue in autism [20].
5. Conclusion: is the amount of aluminium in a vaccine ‘minuscule’?
Simply by looking at just one dose of a vaccine given at 8 weeks of age it is abundantly clear that science does not support this contention, as espoused regularly by many infant paediatricians. In fact, just a single dose of Infanrix Hexa vaccine represents a severe acute exposure to systemically available aluminium. A single dose of this vaccine is equivalent to the exposure to aluminium that an infant would receive from 150 days breast-feeding. It is equivalent to 25 times the daily dose of aluminium received from the most contaminated of infant formulas. It is pertinent to emphasise that an infant would receive a further two doses of this vaccine during the aforementioned 150 day period. It is also highly relevant that other aluminium adjuvanted vaccines, for example Prevenar 13 (https://www.medicines.org.uk/emc/product/453/smpc) and Men B (https://www.medicines.org.uk/emc/product/5168/smpc) are also part of the infant vaccine schedule for this same period. In the United Kingdom it is not uncommon for an infant to receive all three of these aluminium adjuvanted vaccines on the same day. A combined daily exposure of 1.445 mg of aluminium (according to the manufacturer’s data), equivalent to 260 days exposure to aluminium through breast feeding. Exposure to aluminium through a vaccine is, in comparison to diet, an acute exposure and an infant’s physiology will respond differently to exposure to a high concentration of aluminium over a very short time period. The latter, acute versus chronic exposure, while not yet being taken into account in infant vaccination programmes, must now be considered to help to ensure that future vaccination schedules are safe. Currently the EMA and the FDA limit the aluminium content of a vaccine to 1.25 mg (See for example, https://www.ecfr.gov/cgi-bin/text-idx?SID=832c22988b6c802fe810e16ea34ace1a&mc=true&node=se21.7.610_115&rgn=div8). This limit is based upon the aluminium adjuvant’s efficacy in inducing antibody titres. Perhaps now is the time to revise this limit based upon additional factors of vaccine safety.
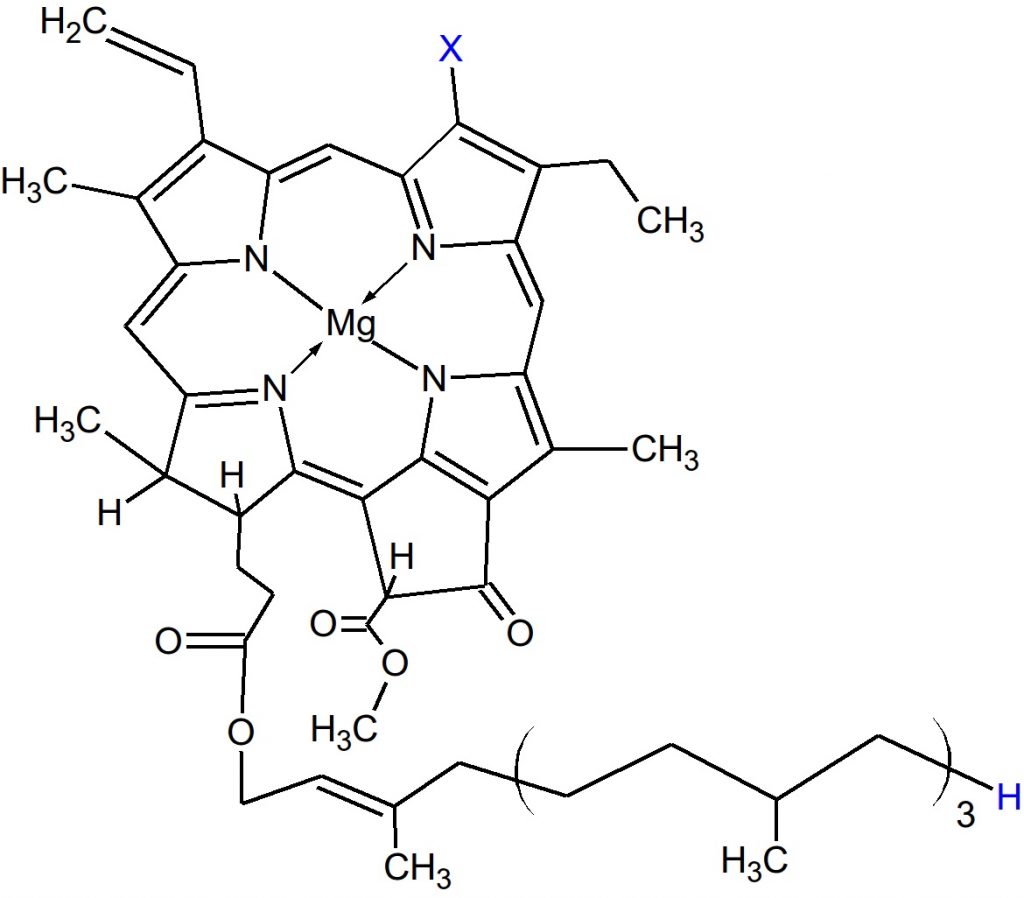
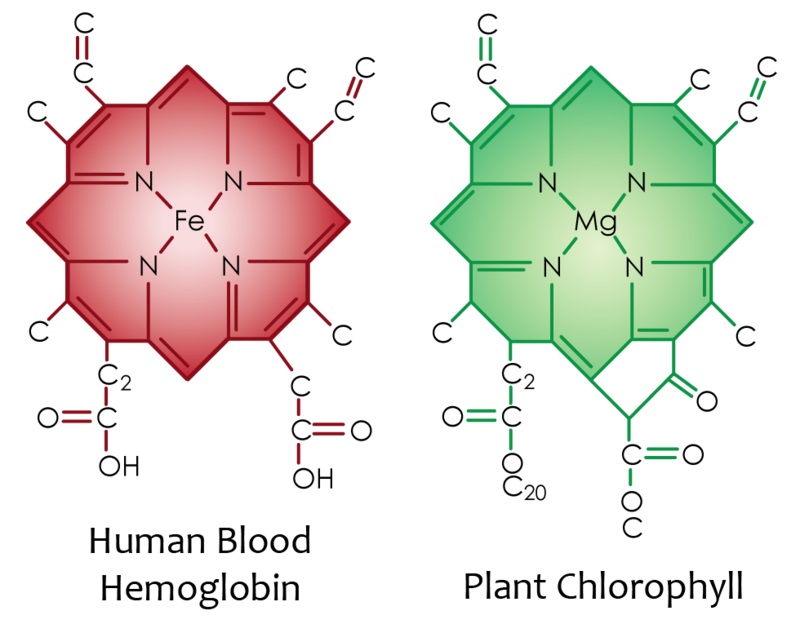
ChooseLife : Here will begin a cursory search into the scientific literature, regarding Magnesium. From the start I should note, that Reams said Chlorophyll was vital to the Liver, that for the Liver to supply the Pancreas with sufficient enzymes for it to regulate sugars properly, we need equivalent to 3oz of green juice daily (probably more nowadays), at the centre of Chlorophyll? Magnesium:
Magnesium is well known for its diverse actions within the human body. From a neurological standpoint, magnesium plays an essential role in nerve transmission and neuromuscular conduction.
It also functions in a protective role against excessive excitation that can lead to neuronal cell death (excitotoxicity), and has been implicated in multiple neurological disorders.
Due to these important functions within the nervous system, magnesium is a mineral of intense interest for the potential prevention and treatment of neurological disorders.
Current literature is reviewed for migraine, chronic pain, epilepsy, Alzheimer’s, Parkinson’s, and stroke, as well as the commonly comorbid conditions of anxiety and depression.
Previous reviews and meta-analyses are used to set the scene for magnesium research across neurological conditions, while current research is reviewed in greater detail to update the literature and demonstrate the progress (or lack thereof) in the field. There is strong data to suggest a role for magnesium in migraine and depression, and emerging data to suggest a protective effect of magnesium for chronic pain, anxiety, and stroke.More research is needed on magnesium as an adjunct treatment in epilepsy, and to further clarify its role in Alzheimer’s and Parkinson’s. Overall, the mechanistic attributes of magnesium in neurological diseases connote the macromineral as a potential target for neurological disease prevention and treatment.
Major depression is a mood disorder characterized by a sense of inadequacy, despondency, decreased activity, pessimism, anhedonia and sadness where these symptoms severely disrupt and adversely affect the person’s life, sometimes to such an extent that suicide is attempted or results.
Antidepressant drugs are not always effective and some have been accused of causing an increased number of suicides particularly in young people.
Magnesium deficiency is well known to produce neuropathologies. Only 16% of the magnesium found in whole wheat remains in refined flour, and magnesium has been removed from most drinking water supplies, setting a stage for human magnesium deficiency.
Magnesium ions regulate calcium ion flow in neuronal calcium channels, helping to regulate neuronal nitric oxide production. In magnesium deficiency, neuronal requirements for magnesium may not be met, causing neuronal damage which could manifest as depression.
Magnesium treatment is hypothesized to be effective in treating major depression resulting from intraneuronal magnesium deficits. These magnesium ion neuronal deficits may be induced by stress hormones, excessive dietary calcium as well as dietary deficiencies of magnesium.
Case histories are presented showing rapid recovery (less than 7 days) from major depression using 125-300 mg of magnesium (as glycinate and taurinate) with each meal and at bedtime.Magnesium was found usually effective for treatment of depression in general use. Related and accompanying mental illnesses in these case histories including traumatic brain injury, headache, suicidal ideation, anxiety, irritability, insomnia, postpartum depression, cocaine, alcohol and tobacco abuse, hypersensitivity to calcium, short-term memory loss and IQ loss were also benefited. Dietary deficiencies of magnesium, coupled with excess calcium and stress may cause many cases of other related symptoms including agitation, anxiety, irritability, confusion, asthenia, sleeplessness, headache, delirium, hallucinations and hyperexcitability, with each of these having been previously documented. The possibility that magnesium deficiency is the cause of most major depression and related mental health problems including IQ loss and addiction is enormously important to public health and is recommended for immediate further study. Fortifying refined grain and drinking water with biologically available magnesium to pre-twentieth century levels is recommended.
Magnesium (Mg) is an essential element for the body. It is a cofactor for ATP, DNA, and RNA and more than 600 enzymes. As it is similar to Ca2+, this element can also act as a cell signaling molecule and play multiple important roles in the nervous, muscle, and immune systems. Recent studies have associated Mg-deficiency with many neurological disorders, such as cerebral vasospasm, Alzheimer’s disease, stroke, and migraine. As it plays such a crucial role in human body, therefore, we summarized the role of Mg in neurological disorders to illustrate the symptoms caused by Mg-deficiency and the possible underlying mechanisms.
METHODS:
We critically discuss the role of it that we review the recent literature of magnesium. We also review the available data which are concerning the role of magnesium in neurological disorders.
RESULTS:
Magnesium is related to neurological disorders on the basis of the study of animals and humans experiments. Furthermore, these nervous systems related diseases include cerebral vasospasm, Alzheimer’s disease, Parkinson’s disease, stroke and migraine.
CONCLUSION:
Magnesium has effects on neurological disorders, such as its utility in cerebral vasospasm, Alzheimer’s disease, Parkinson’s disease, stroke and migraine. So here we make a brief review to conclude it.
Magnesium is the fourth most abundant mineral in the body. It has been recognized as a cofactor for more than 300 enzymatic reactions, where it is crucial for adenosine triphosphate (ATP) metabolism.
Magnesium is required for DNA and RNA synthesis, reproduction, and protein synthesis. Moreover, magnesium is essential for the regulation of muscular contraction, blood pressure, insulin metabolism, cardiac excitability, vasomotor tone, nerve transmission and neuromuscular conduction.
Imbalances in magnesium status-primarily hypomagnesemia as it is seen more common than hypermagnesemia-might result in unwanted neuromuscular, cardiac or nervous disorders.
Based on magnesium’s many functions within the human body, it plays an important role in prevention and treatment of many diseases. Low levels of magnesium have been associated with a number of chronic diseases, such as Alzheimer’s disease, insulin resistance and type-2 diabetes mellitus, hypertension, cardiovascular disease (e.g., stroke), migraine headaches, and attention deficit hyperactivity disorder (ADHD).
Numerous studies have linked severe stress to the development of major depressive disorder (MDD), and suicidal behaviors.
Furthermore, recent preclinical studies from our laboratory and others have demonstrated that in rodents, chronic stress and the stress hormone cortisol has caused oxidative damage to mitochondrial function and membrane lipids in the brain.
Mitochondria play a key role in synaptic neurotransmitter signaling by providing adenosine triphosphate (ATP), mediating lipid and protein synthesis, buffering intracellular calcium, and regulating apoptotic and resilience pathways.
Membrane lipids are similarly essential to central nervous system (CNS) function, because cholesterol, polyunsaturated fatty acids, and sphingolipids form a lipid raft region, a special lipid region on the membrane that mediates neurotransmitter signaling through G-protein coupled receptors and ion channels.
Low serum cholesterol levels, low antioxidant capacity, and abnormal early morning cortisol levels are biomarkers consistently associated with both depression and suicidal behaviors.
In this review, we summarize the manner in which nutrients can protect against oxidative damage to mitochondria and lipids in the neuronal circuits associated with cognitive and affective behaviors.
These nutrients include ω3 fatty acids, antioxidants (vitamin C and zinc), members of the vitamin B family (Vitamin B12 and folic acid) and magnesium. Accumulating data have shown that these nutrients can enhance neurocognitive function, and may have therapeutic benefits for depression and suicidal behaviors. A growing body of studies suggests the intriguing possibility that regular consumption of these nutrients may help prevent the onset of mood disorders and suicidal behaviors in vulnerable individuals, or significantly augment the therapeutic effect of available antidepressants. These findings have important implications for the health of both military and civilian populations.
The aim of this study was to assess the severity of depressive symptoms in postmenopausal women, depending on serum Mg and Zn levels.
The study involved 171 postmenopausal women from Poland, who were not using menopausal hormone therapy (MHT). The intensity of depressive symptoms was evaluated using a standard research technique, the Beck Depression Inventory (BDI).
The plasma Mg and Zn concentrations were measured. Depressive symptoms of different severity levels were diagnosed in 36.8 % of the women. The mean serum Mg level was 1.53 ± 0.28 mg/dL, and Zn level was 72 ±14 μg/dL.
The women with higher serum Mg and Zn levels had less depressive symptoms, and this observation is a precious information which can be used when planning depressive disorder prevention programmes.
Addiction is a dysregulation of brain reward systems that progressively increases, resulting in compulsive drug use and loss of control over drug-taking.
Addiction is a brain disease.
There is evidence that magnesium deficit is involved in addiction to various addictive substances (heroin, morphine, cocaine, nicotine, alcohol, caffeine, and others). Magnesium is involved in all the stages of addiction. Magnesium deficit enhances the vulnerability to psychoactive substance addiction. Stress and trauma reduce the brain magnesium level and at the same time favor addiction development.
In experimental studies, administration of magnesium while inducing morphine dependence in rats reduced the dependence intensity. Magnesium reduces the NMDA receptor activity and the glutamatergic activity. Because stress and trauma induce hypomagnesemia with increased vulnerability to addiction, magnesium intake by people who are under prolonged stress could be a way to reduce this vulnerability and the development of addiction to different psychoactive substances.
Anxiety and depression appear to be associated with increases in drug-related harm and addictive substance use. Magnesium anxiolytic effect could be important for the antiaddictive action. Addiction is characterized by relapses. Magnesium deficiency may be a contributing factor to these relapses.
To study the efficacy and tolerability of 1 g of intravenous magnesium sulfate as acute treatment of moderate or severe migraine attacks.
BACKGROUND:
Migraine is a common disorder in which not only the pain but also the accompanying symptoms such as nausea and vomiting reduce activity and productivity of sufferers. Many drugs used for the treatment of acute migraine attacks have many side effects, are not well tolerated, are ineffective in some patients, or cannot be used during pregnancy or in patients with ischemic heart disease. Magnesium deficiency has been proposed to play a role in the pathophysiology of migraine, and recently treatment of migraine with magnesium has gained considerable interest.
METHODS:
This was a randomized, single-blind, placebo-controlled trial including 30 patients with moderate or severe migraine attacks. Fifteen patients received 1 g intravenous magnesium sulfate given over 15 minutes. The next 15 patients received 10 mL of 0.9% saline intravenously. Those in the placebo group with persisting complaints of pain or nausea and vomiting after 30 minutes also received 1 g magnesium sulfate intravenously over 15 minutes. The patients were assessed immediately after treatment, and then 30 minutes and 2 hours later. Intensity of pain, accompanying symptoms, and side effects were noted.
RESULTS:
All patients in the treatment group responded to treatment with magnesium sulfate. The pain disappeared in 13 patients (86.6%); it was diminished in 2 patients (13.4%); and in all 15 patients (100%), accompanying symptoms disappeared. In the placebo group, a decrease in pain severity but persisting nausea, irritability, and photophobia were noted in 1 patient (6.6%). Accompanying symptoms disappeared in 3 patients (20%) 30 minutes after placebo administration. All patients initially receiving placebo were subsequently given magnesium sulfate. All of these patients responded to magnesium sulfate. In 14 patients (93.3%), the attack ended; in 1 patient (6.6%), pain intensity decreased; and in all 15 patients (100%), accompanying symptoms disappeared. Both the response rate (100% for magnesium sulfate and 7% for placebo) and the pain-free rate (87% for magnesium sulfate and 0% for placebo) showed that magnesium sulfate was superior to placebo. Twenty-six patients (86.6%) had mild side effects which did not necessitate discontinuing treatment during magnesium sulfate administration.
CONCLUSION:
Our results show that 1 g intravenous magnesium sulfate is an efficient, safe, and well-tolerated drug in the treatment of migraine attacks. It is possible that magnesium sulfate could be used in a broader spectrum of patients than other drugs commonly used for attack treatment. In view of these results, the effect of magnesium sulfate in acute migraine should be examined in large-scale studies.
Depression is common, places a large burden on the patient, their family and community, and is often difficult to treat.
Magnesium supplementation is associated with improved depressive symptoms, but because the mechanism is unknown, it is unclear whether serum magnesium levels act as a biological predictor of the treatment outcome.
Therefore, we sought to describe the relationship between serum magnesium and the Patient Health Questionnaire (PHQ, a measure of depression) scores. A cross-sectional analysis of medical records from 3604 adults (mean age 62 years; 42% men) seen in primary care clinics between 2015 and 2018, with at least one completed PHQ were included.
The relationship between serum magnesium and depression using univariate analyses showed a significant effect when measured by the PHQ-2 (−0.19 points/mg/dL; 95% CI −0.31, −0.07; P = 0.001) and the PHQ-9 (−0.93 points/mg/dL; 95% CI −1.81, −0.06; P = 0.037).
This relationship was strengthened after adjusting for covariates (age, gender, race, time between serum magnesium and PHQ tests, and presence of diabetes and chronic kidney disease) (PHQ-2: −0.25 points/mg/dL; 95% CI −3.33, −0.09; P < 0.001 and PHQ-9: −1.09 95% CI −1.96 −0.21; P = 0.015).
For adults seen in primary care, lower serum magnesium levels are associated with depressive symptoms, supporting the use of supplemental magnesium as therapy. Serum magnesium may help identify the biological mechanism of depressive symptoms and identify patients likely to respond to magnesium supplementation.
Type 2 diabetes mellitus is a major global public health problem in the worldwide and is increasing in aging populations. Magnesium intake may be one of the most important factors for diabetes prevention and management. Low magnesium intake may exacerbate metabolic abnormalities. In this study, the relationships of magnesium intake with metabolic parameters, depression and physical activity in elderly patients with type 2 diabetes were investigated.
Methods
This cross-sectional study involved 210 type 2 diabetes patients aged 65 years and above. Participants were interviewed to obtain information on lifestyle and 24-hour dietary recall. Assessment of depression was based on DSM-IV criteria. Clinical variables measured included anthropometric measurements, blood pressure, and biochemical determinations of blood and urine samples. Linear regression was applied to determine the relationships of magnesium intake with nutritional variables and metabolic parameters.
Results
Among all patients, 88.6% had magnesium intake which was less than the dietary reference intake, and 37.1% had hypomagnesaemia. Metabolic syndromes and depression were associated with lower magnesium intake (p < 0.05). A positive relationship was found between magnesium intake and HDL-cholesterol (p = 0.005). Magnesium intake was inversely correlated with triglyceride, waist circumference, body fat percent and body mass index (p < 0.005). After controlling confounding factor, HDL-cholesterol was significantly higher with increasing quartile of magnesium intake (p for trend = 0005). Waist circumference, body fat percentage, and body mass index were significantly lower with increase quartile of magnesium intake (p for trend < 0.001). The odds of depression, central obesity, high body fat percentage, and high body mass index were significantly lower with increasing quartile of magnesium intake (p for trend < 0.05). In addition, magnesium intake was related to high physical activity level and demonstrated lower serum magnesium levels. Serum magnesium was not significantly associated with metabolic parameters.
Conclusions
The majority of elderly type 2 diabetes who have low magnesium intake may compound this deficiency with metabolic abnormalities and depression. Future studies should determine the effects of increased magnesium intake or magnesium supplementation on metabolic control and depression in elderly people with type 2 diabetes.
Sixty percent of cases of clinical depression are considered to be treatment-resistant depression (TRD). Magnesium-deficiency causes N-methyl-d-aspartate (NMDA) coupled calcium channels to be biased towards opening, causing neuronal injury and neurological dysfunction, which may appear to humans as major depression.
Oral administration of magnesium to animals led to anti-depressant-like effects that were comparable to those of strong anti-depressant drugs. Cerebral spinal fluid (CSF) magnesium has been found low in treatment-resistant suicidal depression and in patients that have attempted suicide. Brain magnesium has been found low in TRD using phosphorous nuclear magnetic resonance spectroscopy, an accurate means for measuring brain magnesium. Blood and CSF magnesium do not appear well correlated with major depression.
Although the first report of magnesium treatment for agitated depression was published in 1921 showing success in 220 out of 250 cases, and there are modern case reports showing rapid terminating of TRD, only a few modern clinical trials were found.
A 2008 randomized clinical trial showed that magnesium was as effective as the tricyclic anti-depressant imipramine in treating depression in diabetics and without any of the side effects of imipramine. Intravenous and oral magnesium in specific protocols have been reported to rapidly terminate TRD safely and without side effects.
Magnesium has been largely removed from processed foods, potentially harming the brain.
Calcium, glutamate and aspartate are common food additives that may worsen affective disorders.
We hypothesize that – when taken together – there is more than sufficient evidence to implicate inadequate dietary magnesium as the main cause of TRD, and that physicians should prescribe magnesium for TRD.
Since inadequate brain magnesium appears to reduce serotonin levels, and since anti-depressants have been shown to have the action of raising brain magnesium, we further hypothesize that magnesium treatment will be found beneficial for nearly all depressives, not only TRD.
ChooseLife : Has there ever been a more important time to eat your greens? Make Green Smoothies? Take Epsom Salts baths? or, a few grains of Epsom Salts in drinking water through the day?
This is the best feeling piece of orgonite I have yet experienced.
Somehow the sandwiching of pure yellow and white gold produces a remarkable effect:
relaxing and calming just above the red stone at the peak, and bright an joyful in a region
about the size of a soccer ball just over the physical part of the generator. The centre of
this ball of qi is about 8 inches (20 centimetres) above the bottom of the generator. If
one holds the piece so that this centre of qi lies in ones heart, the feeling there is
quite similar to that which one feels when he collects positive qi there with his
mind. When one hold the generator horizontally in front of the “third eye”
point, it brings a feeling of calm alertness to the head.
~Laozu
***
Don Croft
Rich – That’s a gorgeous, elegant device
***
Hi Rich,
Just picked up the parcel this morning, and it is
absolutely amazing, thank you so much.
The power coming from this thing is
incredible and beautiful
craftsmanship.
Thanks again, P
***
Again, beautifully executed and gorgeous to look at. Makes me feel REALLY good holding – the energy is wonderful, very heart opening. Thank you so much! I think you make by far the best looking HHG’s anywhere!
Blessings and much Love C
***
Rich,
HHG’s are beautiful…and what a wonderful spiral! THANK YOU!
I can feel energy as tingling in my palms…I wanted
to feel orgonite of more skilled and experienced
maker to see if there is any difference.
It is simply pleasant feeling.
I will enjoy every day
these peaces of art!
All the best!
M
***
O M G…..the energy of these devices is amazing!! Even
though I’m not all that sensitive I can feel
the power of your babies – they
are just awesome!!
Could you please tell me what crystals you used, and is the ball
(which looks and feels stunning) different in
composition?
I was going to give some of these pieces away – but I’m not
sure now if I want to part with any of them..
Great craftsmanship and lovely energy.
Thanks a lot, Rich!
All the best Love, C
***
Thanks Rich – I’ve received both parcels this PM.
They all look great – nice work 🙂
RS
***
Thanks Rich, got my parcel yesterday (5th). They’re all wonderful.
Want to keep them all but i’m ment to be spreading
the love.Thank you again for your time
and for sharing your gift.
Take Care, LS
***
Hi Rich,
Just wanted to say the package just arrived and to say a huge Thanks!
They look great and I totally love the purple one 🙂
The rose quartz one too is very nice –
as they all are 🙂
Will check back into your site in future to see what other
colours and designs you are coming up with!
Thanks again!
S
***
Hi Rich,
We have the parcel and the pieces are beautiful. Thank you very
much for the extras; it was terribly kind of you.
Kind regards,
M
***
Hi Rich, My crystal paperweight (generator) arrived last Friday afternoon
and it is beautiful. Wish I felt energy. If its energy
matches its beauty it’s a powerful winner for
sure. I love looking at it and holding it.
Yes, I am delighted with it.
Your workmanship
is exquisite.
Thanks for letting me order it from you.
Thanks ever so much! C
***
Hi Rich,
I am almost speechless! Your package finally arrived!
Your creations are absolutely wonderful!
I am simply amazed – and the
feeling even tops it
all!
I feel really honored to be one of the persons who received HHGs
from you. Thank you again and again
and …
The SBB is also wonderful. I will certainly recommend
you to all my friends who are into orgonite
(which are only few
unfortunately)
All I can say and do is Thank you and send you a boost and
offer to boost you whenever you feel you
need it…
Take care my friend!
~a
***
Hi rich, the 1st parcel arrived today in perfect shape – thanks so much.
Pride of place in my office now – think I will figure out
a way of lighting it to bring out all the work
that’s gone into the
layout 🙂
Thank you again and I look forward to the rest of
them arriving for other
rooms in the
house!
S
***
Dear Mr.Rich,
Your beautiful orgonites have arrived safely yesterday ! But
what a beautiful tool !! You are a terrific artist !!
I am so grateful to you for that you
kindly made me these
beautiful ones…
Anyway thank you very much again and again for
these 12 celestial creations which
you made !!
LOVE LIGHT PEACE
A I
***
Hi Rich. Hope you had a fruitful outing. Just thought I’d let you know about
my trip to see my kiniesiologist friend (kiniesiologist’s aren’t necessarily
energy sensitive but our bodies are). I had disguised the orgonite
(made by you) and an item of equal weight in identical containers
so that when when she placed the containers on me I had no
idea which was which. The first container I didn’t notice
anything in my muscle reflex so I concluded that this
could not be the orgonite, I was then told that the
next container could be the first again or the
second so i wouldn’t set myself up for a
difference. This time I couldn’t feel
anything again so concluded that
this was 1st container (not
orgonite).
My friend informed me that the 1st container had
switched on all my radiant circuits (meridians)
and the 2nd hadn’t. Lo and behold, suprise
suprise the 1st container
had contained
orgonite.
She then tested to see if it was a priority in my life and yes it was.
She then tested some bits that i had made which weren’t
as strong as yours, then she tested to see the best place to
put the orgonite i.e chakra/not chakra, legs,
stomach etc, above head was the outcome
and she placed the orgonite
about 4 inches above
my head.
Well I lasted about 4 seconds before I had to get up from the table laughing
uncontrollably. The sensation was stronger than anything I had
experienced before (and I’ve had a few experiences believe
me). I felt the most enormous rush of supercharged
energy flowing through my head and down my
spine. I didn’t feel I could take it and had
to get away. Of course the laughter
became infectious and my
friend and I
were in
tears.
I had to go for a walk round the block to calm down.
My friend said that she had never
seen anyone react like
that before.
Best.
J
***
Just thought I’d let you know. I went to the mind body spirit exhibition in
London yesterday (nobody had heard of orgonite). I convinced a chap
taking aura photos to take one without and then with me holding the
small hhg made by you. The gentleman seemed a bit ruffled at first
but when he saw the results he was quite amazed as was I. The
first image without the hhg was almost entirely green with a
small brown inclusion on one side. The man said some very
complimentary remarks whilst looking at this image.
Holding the hhg the second image took a while to
settle down flashing all different kind of blue,
eventually settling to a green core
surrounded by blue, he said
this was a significantly
stronger image
than the
first.
J
***
Hi Rich the order arrived today and thank you so much for the
extra orgone cone. That was a nice surprise. They are
fantastic. I hope to buy from you again in a couple
of months now that i want to have one in every
room. My parents have seen them and
my mum’s taken the small one and
put it on the electric
meter.
By the time my sister sees it i think i will have to put in
a bigger order next time. They look marvellous
and i feel abundantly happy.
So big thanks
All The Best
D M
***
They have arrived safely. Absolutely beautiful 🙂
J
***
Hi Rich,
We have recieved the package. They are lovely.
R
***
Hi, Rich!
A note to advise, as promised, that a lovely parcel came in the mail today.
Thank you so very much. How kind and generous of you.
They are both exquisite works of art and possess
a solid smash of heart energy –
uplifting – light. Yes…
Tres, Tres
Jolie.
To quote Croft – “no need for any additional gems in creating
HHG’s for deployment… unless you intend to sleep with
them or drag them to the dinner table with you”
Well, I just might have to do
that with these
beauties.
Wow, Gosh, Holy Doodlebug, Jeepers, Captivating,
Gorgeous, Jolly Good Work, Inspiring, Too
Good to Be True, Can’t Take My
Eyes off of you, etc,
etc…
the list of superlatives could certainly go on.
Thanks, Rich.
Take good care.
D K
***
Hi Rich,
I got the generators in the post today & I must say they look stunning.
Thanks again,
B C
***
Cesco
Rich probably makes some some of the nicest generators
I have seen, well worth
getting
***
Laozu (Early Observation)
Rich’s creations, besides being beautiful, are quite
good in the quality of qi. He is oneof the most careful people
I know in makingorgonite.
***
Gifting,
Renegades Of Junk!
Areas Gifted (amounts are guestimates);
Bournemouth, Poole, Christchurch, Ferndown etc 1000+ TB’s HHg’s Dorchester, Weymouth, Blandford Forum et al 500+ TB’s HHg’s Worcester 400+ TB’s HHg’s Exeter 150 TB’s South West to Central London 1000+ TB’s HHg’s Isle Of Wight 250 TB’s Scottish Sites (Schiehallion, Fortingall, Rosslyn etc) 150 TB’s HHgs Southampton 100 TB’s
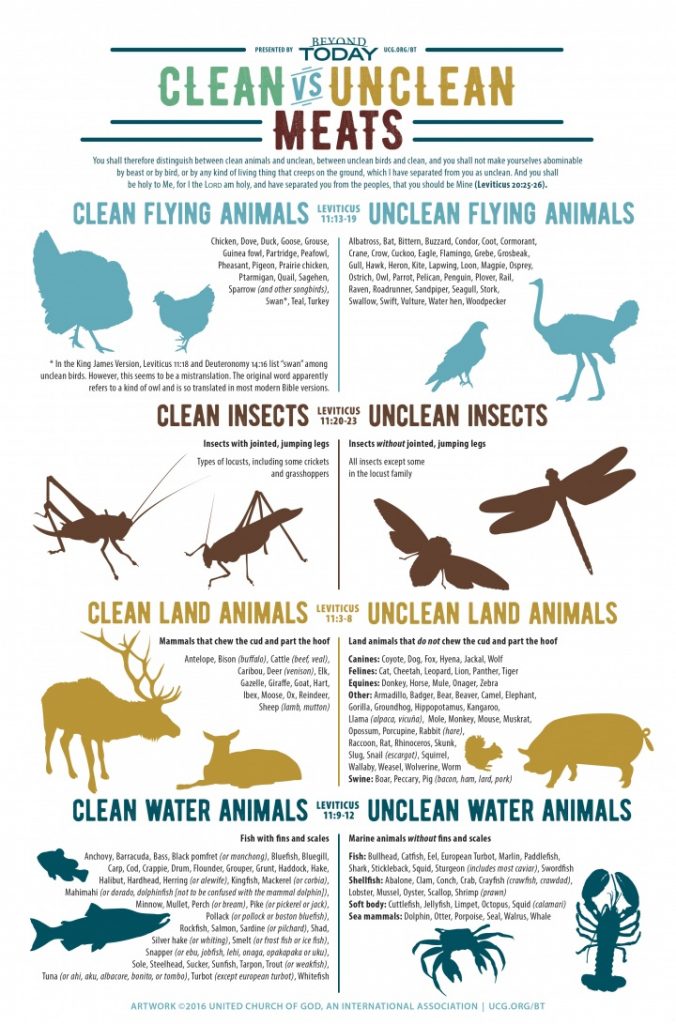
When reading about the diets of others, I kept coming across this concept of clean meats, but never took any time to learn (long term Vegetarian).
However, now my girls are being raised on a diet with Animal matter, I find it much better to understand what may help, or, potentially harm my daughters vitality and growth.
So, we have the concept of “Clean Meats” as stated in Leviticus:
Not a recommendation of safety by ChooseLife. Perhaps, for the author, less unsafe!
Now, alone this may be of great benefit, some may still find they do not feel good at all on meat. However for those who feel the need for animal matter in their diet, enter Dr Reams :
Dr Reams:
For six weeks I did tests on him, without any limiting of his diet whatever. And he was slowly getting worse. I took that information then and began to weigh it out, day by day by day.
I found out then, every day that he ate the unclean foods such as catfish, shrimp, lobster, pork, ham, bacon, sausage, pork chops, spare ribs, or whatnot, his energy dropped. In the other days, it either held its own or kind of gained a little. It’s so much easier to bring it down than it is to bring it up.
So what I found out was that the unclean meats digest in a period of three hours and the clean meats in a period of 18 hours average. Now that is a difference! When meats digest too fast, they throw too much high-powered energy into your system at one time, and it burns you up. I have seen many people in their late thirties or early forties. To look at them, you’d think they were in their late seventies because they had eat so much high-powered foods, until it burned them up.
Flaxseed (FS) is a nutritional supplement with high concentrations of (n-3) fatty acids and lignans that have anti-inflammatory and antioxidant properties. The use of FS in the prevention or treatment of acute lung disease is unknown. In this study, we evaluated diets with high FS content in experimental murine models of acute lung injury and inflammation. The kinetics of lignan accumulation in blood, following 10% FS supplementation, was determined using liquid chromatography tandem mass spectrometry. Mice were fed isocaloric control and 10% FS-supplemented diets for at least 3 wk and challenged by hyperoxia (80% oxygen), intratracheal instillation of lipopolysacharide, or acid aspiration. Bronchoalveolar lavage was evaluated for white blood cells, neutrophils, and proteins after a 24 h postintratracheal challenge of hydrochloric acid or lipopolysacharide, or after 6 d of hyperoxia. Lung lipid peroxidation was assessed by tissue malondialdehyde concentrations. The plasma concentrations of the FS lignans, enterodiol and enterolactone, were stable after mice had eaten the diets for 2 wk. Following hyperoxia and acid aspiration, bronchoalevolar lavage neutrophils decreased in FS-supplemented mice (P = 0.012 and P = 0.027, respectively), whereas overall alveolar white blood cell influx tended to be lower (P = 0.11). In contrast, neither lung injury nor inflammation was ameliorated by FS following lipopolysacharide instillation. Lung malondialdehyde levels were lower in hyperoxic mice than in unchallenged mice (P = 0.0001), and decreased with FS treatment following acid aspiration (P = 0.011). Dietary FS decreased lung inflammation and lipid peroxidation, suggesting a protective role against pro-oxidant-induced tissue damage in vivo.