This study involved a randomized, controlled, single-blind 12-month treatment study of a comprehensive nutritional and dietary intervention.
Participants were 67 children and adults with autism spectrum disorder (ASD) ages 3-58 years from Arizona and 50 non-sibling neurotypical controls of similar age and gender.
Treatment began with a special vitamin/mineral supplement, and additional treatments were added sequentially, including essential fatty acids, Epsom salt baths, carnitine, digestive enzymes, and a healthy gluten-free, casein-free, soy-free (HGCSF) diet.
There was a significant improvement in nonverbal intellectual ability in the treatment group compared to the non-treatment group (+6.7 ± 11 IQ points vs. -0.6 ± 11 IQ points, p = 0.009) based on a blinded clinical assessment.
Based on semi-blinded assessment, the treatment group, compared to the non-treatment group, had significantly greater improvement in autism symptoms and developmental age. The treatment group had significantly greater increases in EPA, DHA, carnitine, and vitamins A, B2, B5, B6, B12, folic acid, and Coenzyme Q10.
The positive results of this study suggest that a comprehensive nutritional and dietary intervention is effective at improving nutritional status, non-verbal IQ, autism symptoms, and other symptoms in most individuals with ASD. Parents reported that the vitamin/mineral supplements, essential fatty acids, and HGCSF diet were the most beneficial.
In 1984, as an undergraduate at the University of Stirling, Scotland and while carrying out my first piece of independent research, I watched for the first time a fish, a salmon parr, die from acute aluminium toxicity. The whole process took less than forty-eight hours. Within six hours, the fish showed signs of distress and its behaviour changed markedly. It proceeded to seek out the corners of the tank, pushing its head and body against the side of the tank. After twenty-four hours, it began to move randomly and chaotically around the tank before losing its orientation, slipping onto its back, taking a last gasp, before dying. I was left in no doubt about the toxicity of aluminium. I am recalling this event herein because there does seem to be significant complacency concerning the toxicity of aluminium.
An Aluminium Adjuvant is Acutely Toxic Too
In a recent post (https://www.hippocraticpost.com/pharmacy-drugs/the-toxicity-of-aluminium-adjuvants/) I explained why a single injection of a vaccine that includes an aluminium adjuvant is, akin to the salmon above, also an acute exposure to aluminium. It is acute because the total concentration of aluminium in the immediate vicinity of the injection site is extremely high, in the case of a single dose of Infanrix Hexa vaccine, approximately 8000 times higher than is required to kill a salmon parr within forty-eight hours. Even allowing for some dilution of the injected aluminium adjuvant into body fluids bathing and innervating the tissues surrounding the injection site the total concentration of aluminium in a vaccine is sufficient to cause cell death within hours and perhaps minutes of receiving the injection. This is the definition of an acute response, death (cells or whole organism) within a short period of exposure to a toxin. It is a necrotic form of cell death. It initiates an inflammatory response (redness at the injection site). This inflammation drives and perhaps accelerates the subsequent immune response (https://www.hippocraticpost.com/infection-disease/safety-concerns-aluminium-adjuvants/).
A number of mechanisms bring about remediation of acute aluminium toxicity at a vaccine injection site. These are chemical, physical and biological. The toxic free metal ion, Al3+, forms soluble and insoluble complexes with myriad biological molecules while particles of aluminium adjuvant and other insoluble aluminium compounds are taken up by cells infiltrating the vaccine injection site. All of these processes act to reduce the acute toxicity of aluminium at the injection site by lowering the immediate concentration of toxic Al3+. These remedial processes act to secure aluminium in a number of different compartments. All are systemic and all are potential sources of biologically reactive aluminium to the rest of the body. Many chemical compartments where aluminium is bound in myriad different complexes including simple organic moieties like citrate or more complex proteins like the iron transport protein transferrin promote the transport of aluminium away from the injection site.
These processes can be envisaged as continuous passive diffusion of soluble aluminium away from the injection site. The majority of injected aluminium adjuvant is particulate in the first instance and actively taken up, literally eaten, by a number of different cells infiltrating the injection site. Some particles of aluminium adjuvant are taken up by macrophages and thereafter they are retained at or close to the injection site as a granuloma. Generally, these collections of macrophages are considered as benign ‘cancers’ though such descriptions have been coined for situations where the cellular cargo is not aluminium. For example, macrophagic myofasciitis or MMF is a disease, first described by Romain Gherardi in Paris, in which aluminium-rich granulomas at vaccine injection sites are implicated in disease aetiology. Other cells heavily laden with aluminium do not remain close to the injection site and carry their cargo well beyond where the vaccine is administered, for example visiting local lymph nodes as early stops on their travels. Evidence is mounting that these cells may transport aluminium into brain tissue using both lymph and blood as access routes. Perhaps most worrying, evidence of transport of aluminium into brain tissue across the blood-brain barrier and meninges has been shown in autism (https://www.hippocraticpost.com/infection-disease/aluminium-and-autism/).
An Aluminium Adjuvant is a Significant Exposure to Aluminium
With reference to my recent post, an aluminium adjuvant in a vaccine is an acute exposure to aluminium at the vaccine injection site. However, the aluminium content of a single vaccine also represents a significant exposure to aluminium in an infant. For example, the injection of a single dose of Infanrix Hexa into an infant is equivalent to 164 times the daily dose of aluminium in breast milk feeding. Even allowing for an unrealistically high proportion of aluminium being retained in a granuloma at the vaccine injection site (say, for example 40% of the injected aluminium) the daily dose of aluminium in Infanrix Hexa is 100 times higher than an infant receives in breast-feeding. This is a high exposure to aluminium and inevitably results in aluminium being retained in an infant’s tissues, including the infant brain. This is why we must not be complacent about the use of aluminium adjuvants in vaccines. It is why there should be regulations based upon the toxicity of aluminium that govern how much aluminium is allowed in a single vaccine. This limit should be used to give clear unequivocal advice on the number of vaccines that include an aluminium adjuvant that can be given within a specified period. Aluminium is only toxic (as opposed to essential) in the human body and so we should always take every possible step to reduce exposure and ultimately the body burden of aluminium. Infants, due to increased gastrointestinal absorption, reduced urinary excretion and a developing blood-brain-barrier, are uniquely vulnerable to aluminium. We need to protect them from their future now.
Professor in Bioinorganic Chemistry Keele University Honorary Professor, UHI Millennium Institute Group Leader – Bioinorganic Chemistry Laboratory at Keele
Aluminium salts are common adjuvants in vaccines given to children. Their physical, chemical and biological properties have recently been reviewed [1]. However, a debate continues as to whether neonate and infant exposure to aluminium through vaccination is biologically significant with respect to their exposure to aluminium through other routes and especially diet. For example, paediatricians, responsible for administering the vaccine schedule for children, seem in particular, to be uninformed about the properties of aluminium adjuvants and their mode of action in vaccines. This apparent ignorance of the published scientific literature is unexpected in those charged with the wellbeing of neonates and infants and especially in the light of Janeway’s description of alum adjuvant as ‘the immunologist’s dirty little secret’ [2]. Paediatricians such as recently (07/04/2019) Andrew Pollard in The Sunday Times, have a habit of reverting to pure ‘baby talk’ when for example; describing how much aluminium is present in an infant vaccine. They use terms such as ‘minuscule’ and ‘teeny-weeny’ to tell anyone, who asks, how little aluminium there is in a vaccine. They usually then proceed to compare the amount of aluminium in a vaccine with the amount of aluminium in (an adult’s) diet. There are, of course, more accurate, understandable ways to inform parents and other interested parties how much aluminium is present in a vaccine, and I shall endeavour to achieve this herein. An appreciation of how much aluminium is present in a single injection of a vaccine is critical to understanding how aluminium adjuvants are effective in stimulating the immune response.
2. How much aluminium is found in vaccines?
Currently about 20 childhood vaccines include an aluminium adjuvant. Vaccine industry literature (for example; https://www.medicines.org.uk/emc/product/2586/smpc) expresses the aluminium content of an individual vaccine as an amount (weight) of aluminium (not aluminium salt) per unit volume of a vaccine (usually 0.5 mL). Industry does this to account for the fact that there are no strict molecular weights for the polymeric aluminium salts that are used as adjuvants in vaccinations. They prepare acid digests of the adjuvants and measure their total aluminium using ICP MS. This is not explained in the literature they provide with vaccines and can cause confusion for some as the actual weight of hydrated aluminium salt (e.g. aluminium oxyhydroxide, aluminium hydroxyphosphate and aluminium hydroxyphosphatesulphate) in any vaccine preparation is actually approximately ten fold higher. The aluminium salt is the major component of a vaccine (after water) and its high content is why vaccine preparations are invariably cloudy in appearance [1]. As an example, GlaxoSmithKline’s Infanrix Hexa vaccine is reported by the manufacturer to contain 0.82 mg of aluminium per vaccine (0.5 mL). Thus, the weight of aluminium salt in this vaccine is approximately 8 mg, which is approximately ten times the weight of all of the other components of the vaccine when combined. An aluminium-adjuvanted vaccine is essentially a very high concentration of an aluminium salt (8 mg/0.5 mL or 16 mg/mL or 16 g/L) in which just μg of other vaccine components including antigens and other excipients are occluded.
3. Is the amount of aluminium in a vaccine ‘minuscule’?
Generally, in the United Kingdom the first dose of Infanrix Hexa vaccine is injected into muscle when an infant is 8 weeks old. All 8 mg of the aluminium salt (or 0.82 mg of aluminium) will immediately be systemic; it is inside the infant’s body. The repercussions of this being that the injected aluminium may only leave the body through its excretion in either the infant’s urine or sweat. What is the immediate biological response to this exposure to aluminium adjuvant? Aluminium is described as a silent visitor to the human body. What this means is that in the evolution of life on Earth and latterly human evolution, no historic signature is found as evidence for previous exposure to aluminium [3]. By way of comparison with another toxic and non-essential metal, if the adjuvant used in a vaccine was composed of a cadmium salt its injection would immediately initiate a counter-response by the body in an attempt to remove the toxicant. Proteins known to bind and help in the detoxification of cadmium are produced and this is a sure sign that biochemistry had previously encountered non-essential cadmium and selected it out of essential biochemical pathways. Such restorative attempts at detoxification are not triggered for biologically available aluminium and so the ‘processing’ of aluminium adjuvant at the injection site of a vaccine is completely adventitious and one might suggest, random and chaotic. The latter because the fate of aluminium in the body, unlike essential and other non-essential metals, is not subject to any form of homeostasis. Myriad chemical and biological processes will initiate the slow redistribution of the injected aluminium throughout the infant’s body. These steps will involve the processes of disaggregation, dissolution, complexation, precipitation, distribution, cellular uptake and translocation. The description of each one of these processes is an essay in itself and we have addressed them all in many complementary publications [1]. An important and vaccination-specific distinction to make at this point and to carry forward to the following discussion is that aluminium injected into muscle as an adjuvant in a vaccine potentially has uninterrupted access to the infant brain. This is because there is no prerequisite for its passage via the liver, the most prominent organ of detoxification in humans.
We asked if 0.82 mg of systemically available aluminium administered as a single dose in a vaccine is, as some paediatricians would suggest, a minuscule amount of aluminium, for example, as compared to aluminium in the diet. Infants receiving Infanrix Hexa vaccine at 8 weeks of age are concurrently either being breast or formula fed. Data show that the former is likely to result in an 8 week old infant ingesting up to 0.1 mg of aluminium each day [4,5]. On the day an infant receives 8 mg of an aluminium salt, or 0.82 mg of aluminium, in a vaccine it will also ingest 0.1 mg of aluminium in breast milk. However, what proportion of this 0.1 mg of dietary aluminium will be absorbed across the infant gut? Previous research has asked a similar question [6]. The reality is that data for the absorption of aluminium across the infant gut do not presently exist and one has to apply gastrointestinal absorption data obtained for adults. The oft-cited value for adults is that less than 0.1% of ingested aluminium in diet is actually absorbed [7]. The infant gut at 8 weeks is incomplete [8] and is likely to be much more permeable to dietary aluminium, perhaps as much as 100 times more permeable. Applying such clearly conditional criteria it can be estimated that 10% of ingested aluminium or 0.01 mg/day of aluminium in breast milk is absorbed across the infant gastrointestinal tract. However, the blood carrying nutrients and toxins that have been absorbed from the gut, to the rest of the body must first pass through the liver, the major detoxification system of the body. Data on the efficiency of the liver in removing aluminium from the blood is, at best, incomplete in adults [9] and completely unknown in infants. If it is estimated that the liver is 75% efficient in this respect for adults then it is probably only 50% efficient in an infant. When these various conditional factors are accounted for it can be estimated that an infant’s exposure to systemically available aluminium from breast-feeding is approximately 0.005 mg of aluminium each day. In essence during the first 8 weeks or 56 days of life, breast-feeding ostensibly drip feeds an infant with a combined total of 0.28 mg of systemically available aluminium. On day 56 the infant receives a single dose of 0.82 mg of aluminium in the Infanrix Hexa vaccine, a dose equivalent to 3 times the amount of aluminium the infant received during the entire 55 days of life prior to its vaccination. It is well known, if highly unfortunate, that infant formulas are heavily contaminated with aluminium [10,11] and in a worst-case scenario an infant only being formula-fed from birth might be exposed to 0.030 mg of aluminium each day up to vaccination on day 56. Even in this worst-case scenario, the exposure to systemically available aluminium on vaccination day is 25 times higher through the vaccine than through the diet.
4. Acute versus chronic exposure to aluminium
Breast or formula feeding in an infant is a chronic exposure to aluminium. The infant is exposed to a small but continuous supply of systemically available aluminium, aluminium that has the potential to be stored in the infant’s body and excreted from the infant’s body in the urine. Perhaps, at no point during continuous chronic (drip feed) exposure in infancy (0–12 months of age) does the concentration of aluminium in any one physiological compartment increase to bring about overt toxicity. How does dietary exposure to aluminium in infants compare to exposure through vaccination, for example, a single Infanrix Hexa vaccine at 8 weeks of age? The concentration of aluminium (not aluminium salt) in an Infanrix Hexa vaccine upon its injection into muscle is, according to the manufacturer, 0.82 mg/0.5 mL or 1.64 mg/mL or 1.64 g/L or approximately 60 mmol/L. This is the concentration of total systemically available aluminium immediately present at the injection site of the vaccine and available to bring about biological effect. Aluminium adjuvants are not inert depots at the vaccine injection site; they are sources of biologically reactive aluminium [1]. This concentration of total aluminium at the injection site of a vaccine can be put into context by examining the cellular toxicity of aluminium [12] and specifically as identified in recent scientific publications. We can ask the question if we would expect this concentration of aluminium to produce biological effects including cell death at the vaccine injection site. A relevant cell to investigate are lymphocytes and research has demonstrated significant genotoxicity in lymphocytes exposed to only 0.020 mmol/L total aluminium [13]. Similarly, in another study using lymphocytes 0.6 mmol/L total aluminium resulted in significant immunosuppression in both T and B-lymphocytes [14]. Clearly, we would expect profound effects on lymphocytes at the injection site of a vaccine where the total aluminium concentration is 60 mmol/L. Macrophages, a characteristically robust cell, are susceptible to aluminium toxicity demonstrating 50% cell death at a total aluminium concentration of 10 mmol/L [15]. Other more sensitive cell lines would include neuroblastoma where cell viability is reduced by 50% by less than 1 mmol/L total aluminium [16] and similarly for primary hippocampal neurons exposed to only 0.05 mmol/L total aluminium [17]. The concentration of systemically available aluminium immediately present at the injection site of a vaccine is very high in comparison to studies on cell cytotoxicity in the scientific literature. It is an acute exposure to aluminium and it results in significant cytotoxicity including necrotic cell death [1]. The resulting tissue inflammation is the characteristic red mark on the skin at the injection point. This acute toxicity in the immediate vicinity of the injection site underlies the success of aluminium salts as adjuvants in vaccinations [1]. However, while some cells, both present at and infiltrating the injection site, are compromised and especially immediately, other cells act to remedy the situation by taking up aluminium adjuvant into their cytoplasm [18]. This action reduces the concentration of biologically reactive (toxic) aluminium at the injection site and locks away potentially cytotoxic aluminium in intracellular vesicles. Herein may be the real issue linking aluminium adjuvants and severe adverse events following a vaccine. These aluminium-loaded cells remain viable for days, potentially weeks, which means that they can transport their cargo of aluminium anywhere in the body including the infant brain. The recruitment of systemic cells including macrophages to the central nervous system is a widely documented phenomenon [19]. There is now a viable mechanism for the accelerated loading of an infant’s brain with aluminium and evidence to support such a mechanism was demonstrated in our recent paper on aluminium in brain tissue in autism [20].
5. Conclusion: is the amount of aluminium in a vaccine ‘minuscule’?
Simply by looking at just one dose of a vaccine given at 8 weeks of age it is abundantly clear that science does not support this contention, as espoused regularly by many infant paediatricians. In fact, just a single dose of Infanrix Hexa vaccine represents a severe acute exposure to systemically available aluminium. A single dose of this vaccine is equivalent to the exposure to aluminium that an infant would receive from 150 days breast-feeding. It is equivalent to 25 times the daily dose of aluminium received from the most contaminated of infant formulas. It is pertinent to emphasise that an infant would receive a further two doses of this vaccine during the aforementioned 150 day period. It is also highly relevant that other aluminium adjuvanted vaccines, for example Prevenar 13 (https://www.medicines.org.uk/emc/product/453/smpc) and Men B (https://www.medicines.org.uk/emc/product/5168/smpc) are also part of the infant vaccine schedule for this same period. In the United Kingdom it is not uncommon for an infant to receive all three of these aluminium adjuvanted vaccines on the same day. A combined daily exposure of 1.445 mg of aluminium (according to the manufacturer’s data), equivalent to 260 days exposure to aluminium through breast feeding. Exposure to aluminium through a vaccine is, in comparison to diet, an acute exposure and an infant’s physiology will respond differently to exposure to a high concentration of aluminium over a very short time period. The latter, acute versus chronic exposure, while not yet being taken into account in infant vaccination programmes, must now be considered to help to ensure that future vaccination schedules are safe. Currently the EMA and the FDA limit the aluminium content of a vaccine to 1.25 mg (See for example, https://www.ecfr.gov/cgi-bin/text-idx?SID=832c22988b6c802fe810e16ea34ace1a&mc=true&node=se21.7.610_115&rgn=div8). This limit is based upon the aluminium adjuvant’s efficacy in inducing antibody titres. Perhaps now is the time to revise this limit based upon additional factors of vaccine safety.
Why is it, that many modern diseases of high prevalence, affect some people and not others?
Well? It can’t be the Mercury, they said, as otherwise everyone would get it.
Well? It can’t be the Fluoride, our body needs and produces that.
Well? It can’t be the Aluminium, it’s prevalence means we have historical digestive capability to cope they say, it is such tiny amounts given medically they say.
Well? It can’t be poor diet, the body has homeostasis to set right such problems.
Until we start to look at life from another perspective, illness may hurtle towards us, regularly, with ever more velocity. Given the continual decline in soil quality, producing less vital fruits, vegetables, meats, nuts and seeds (even herbs). The problem is exacerbated by the emergence of processed sugars and flours, which in most guises are antagonistic to our biochemistry, chiefly Calcium (Magnesium, Iodine et al.), which might make a simple walk in the park dangerous, simply a cut or graze might cause an infection.
When fluids in the endosome become too acidic, the cargo is trapped within the endosome deep inside the cell. When the endosome contents are more alkaline, the cargo lingers at the cell’s surface for too long.
They found that mouse cell lines containing the Alzheimer’s disease gene variant had more acidic endosomes (average of 5.37 pH) than cell lines without the gene variant (average of 6.21 pH).
Pretty compelling picture.
The above research, clearly demonstrate that it is when pH of matter falls (or rises) out of its environmental bounds, matter starts to decay and becomes unable to buffer stronger opposing electromagnetic forces, demonstrated by the papers above showing it is pH dropping which really appears to make Mercury, Aluminium & Fluoride (Excessively) Toxic, even in the ‘low’ amounts suggested as safe by regulatory authorities.
This ticks all the boxes of “why some and not others” with Dental Amalgam, Vaccination related side effects (Aluminium Hydroxide pH 9.5 injected into an individual with a tissue pH in the 5.0-5.5 range is hugely more dangerous than an individual in the safer zone of 6-7 – the author believes this is the propellant of many debilitating diseases, the data presented in this article supports this theory).
So, we have a period eating poorly, high sugars, processed carbs, processed meats/dairy. Any part of this combination, as a core part of diet, to the wrong individual, will make the tissue pH plummet, it is all there in the studies. If individuals live like this, then the smallest of environmental pollutants may become lethal (because we lack the buffer system, which may allow the host sufficient robustness to cope, this is what gives the lymphatic system the traction to cycle these toxins out).
If you raise the pH of your terrain (eat more greens & more Omega 3!), you suddenly become less prone to infection and heavy metals become less toxic to you, it is almost like God was trying to pass a message to humanity through Carey Reams, isn’t it?
Higher Fruit and Vegetables, less meat, 22,000 people studied, raises pH of Urine:
In conclusion, a more alkaline diet, higher fruit and vegetable and lower meat intake were related to more alkaline urine with a magnitude similar to intervention studies
CONCLUSIONS: Low urine pH is significantly associated with abnormal glucose tolerance; therefore, measuring urine pH might prove useful for identifying patients at high risk for diabetes.
Simply testing someones pH, may show clearly whether they have the biological capability, at all, to repel these neurotoxins, could life be so simple? (not that I advocate vaccination at all personally, or any unnecessary exposure to these nasty elements, full stop). However, If I was a worried parent, before deciding on vaccination I would test my childs urine pH, to get an indicator the gravity of danger my child faces.Then if their pH was below 6.0 maybe feed them more greens and good oil for a few weeks, test again, then make a more informed decision. This seems eminently sensible.
ChooseLife : pH balancing is the middle path. Developed from thoughts of Randall David Dew, it is time this great man was set free.
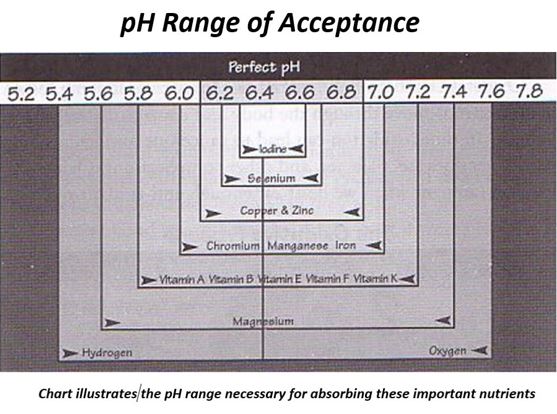
To note, the pH of the ‘high fruit and vegetable diet’, is higher than Carey Reams suggested we should attain, to produce perfect friction (or metabolic energy release between anionic and cationic elements in the body), he suggests 6.4 is perfect urine pH, the same for Saliva pH, which together denote the overall pH terrain status (the mean of 2x Urine 1x Saliva).
As the studies above all show, once your pH is in the range below 5.5 biological function becomes very difficult to sustain, without disease and illness. This dovetails Carey Reams profound teachings about Biological Ionisation, where he demonstrated multiple nutrients cannot be absorbed when the terrain is in this low pH condition (or excessively high also, as shown).
Literature Review: Six long-term chronic toxicity studies to two species of aquatic invertebrates(Ceriodaphnia dubia and Daphnia magna) were identified as acceptable studies.
See Table # “Overview of long-term effect on aquatic invertebrates” (below). ECr10s were calculated using raw data provided from each study using the statistical program Toxicity Relationship Analysis Program (TRAP) version 1.10 from the US EPA National Health an Environmental Effects Research Laboratory (NHEERL).
All other endpoints were as reported in each study. NOECs and EC10s ranged from 0.076 to 4.9 mg Al/L and 0.021 to 0.997 mg Al/L, respectively. Water quality data for these studies suggest a direct relationship between toxicity and pH, hardness, and DOC. For studies that experimentally manipulated water quality (e.g., CIMM 2009 and 2010a ), toxicity decreased with increasing pH, hardness, and DOC.
Aluminum and water: reaction mechanisms, environmental impact and health effects
Aluminum naturally occurs in waters in very low concentrations. Higher concentrations derived from mining waste may negatively affect aquatic biocoenosis. Aluminum is toxic to fish in acidic, unbuffered waters starting at a concentration of 0.1 mg/L. Simultaneous electrolyte shortages influence gull permeability, and damage surface gull cells. Aluminum is mainly toxic to fish at pH values 5.0-5.5. Aluminum ions accumulate on the gulls and clog these with a slimy layer, which limits breathing. When pH values decrease, aluminum ions influence gull permeability regulation by calcium. This increases sodium losses. Calcium and aluminum are antagonistic, but adding calcium cannot limit electrolyte loss. This mainly concerns young animals. An aluminum concentration of 1.5 mg/L turned out to be fatal to trout. The element also influences growth of freshwater bony fish.
Choose Life : Considering what is happening in the world in these times, these studies about aquatics, helps link so much together. This post will be updated as I find more data on this, just started a new job so bare with me please.
Conclusions : The etiology and pathogeneis of ASD are not well understood. Autism Spectrum Disorders comprise a complex of clinical syndromes found predominantly in infants and younger people consisting of disturbances in cognition and comprehension, communication disorders, epilepsy, and behavior that have an underlying common pathology of neurodegeneration of the cerebellar Purkinje cells and other areas of the brain. Other studies in humans have shown chronic inflammatory changes in the brain, particularly in the cerebellum, and involvement of the microglia in this pathology.
Our review presents evidence suggesting a hypothesis unifying the syndromes in ASD. The clinical as well as pathological findings of the ASD have a set of pathological events with the common denominator being immunoexcitotoxicity leading to neurodegeneration and abnormalities in the connectome, particularly in developing brains in the neonate and young with evidence that explains the clinical presentation of ASD.
Our hypothesis is supported by experimental evidence from animal models and by some clinical testing and pathology studies that give credibility to the concept of immunoexcitotoxicity as the underlying cause of ASD. A great number of conditions can trigger both the inflammatory and the excitotoxic cascade, including sequential vaccination, infections, hypomagnesemia, ROS, RNS and LPP, fluoride and Al3+ as well as a number of other neurotoxic metals and industrial chemicals. Chronic activation of the brain’s immune system increases extracellular glutamate levels sufficiently to trigger the excitotoxic cascade, which in conjunction with inflammatory cytokines and prostaglandins, magnifies the damaging effects of both. This mechanism explains most of the features of the ASD, including the behavioral difficulties, language problems, repetitive behaviors, intellectual delay, and episodic dyscontrol of anger. In addition, these mechanisms explain the pathological findings as well, including the changes in the cerebellum, abnormalities in connectivity and the widespread activation of microglia and astrocytes. It also explains why ASD has not disappeared despite the removal of mercury from most childhood vaccines, since excessive immune activation is the initiating and sustaining event in ASD. Evidence is presented that the abundance of fluoride added to the water worldwide and the widespread availability of aluminum particularly to infants and young children through aluminum containing vaccinations, singly or together as aluminofluoride can be potent factors in producing the condition of immunoexcitotoxicity that leads to the pathological changes seen in ASD. The vaccination program should be evaluated to reduce the excessive stimulation of immature immune system and to replace Al3+-adjuvants.
We have also reviewed studies that indicate that fluoride and Al3+, as ubiquitous environmental and food-derived toxins, can exacerbate the pathological and clinical problems of ASD. In synergistic action as AlF4− these elements induce numerous chronic pathophysiological consequences at several times lower concentrations than either Al3+ or fluoride acting alone. AlF4− may evoke several signaling disorders and act as an endocrine disruptor. Moreover, most of the excitotoxic events may enhance the subclinical pathological alterations and/or the genetic susceptibility seen in ASD. The full genetic potential of the child for brain and mental development may be also compromised due to deficiency of micronutrients.
Our immunoexcitotoxic hypothesis opens the door to a number of new modes of prevention and amelioration of ASD. Elimination of various sources of fluoride and Al3+ in early development and consumption of a diet containing essential nutrients and antioxidants have been shown to be beneficial to brain function. As a multifaceted disorder, ASD requires a multifaceted approach, one that should include the protection against excitotoxicity, as well as the protection against microglial activation.
There are several experimental studies that can be constructed to test the immunoexcitotoxic hypothesis, especially as regards vaccines. Such a study would require the use of non-human primates at various stages of development, from intrauterine life to early post-natal development corresponding to human neurodevelopment during vulnerable neurodevelopmental milestones. The study would follow the vaccine schedules used with human newborns and pre-schoolers. One would need to use the exact vaccines used in the human vaccine schedules but of comparable doses based on weight.
To measure microglial activation in response to the vaccines, it would be necessary to use microglial activation PET scanning techniques at various time schedules before and following the vaccines. Newer microglial activation PET scanning techniques are being developed that hold the possibility of differentiating between M1 and M2 microglial activation phenotypes. Long-term follow-up scanning would be necessary to delineate prolonged microglial activation as has been observed in cases of autism. Measure of glutamate levels in the affected areas of the brain should also be conducted, perhaps in a separate set of monkeys to prevent inadvertent activation of local microglia. More extensive studies could be envisioned, such as measures of EAATs, glutaminase, and NADPH oxidase within affected brain areas in response to vaccination.
In addition, studies should be conducted measuring the aluminum, fluoride and aluminofluoride complex concentration in the affected areas of the brain in autopsied cases of autism. This should include the various cell types as well as cellular compartments. This could also be done experimentally in the non-human primate studies using human vaccines described above. Controls could establish the levels of these toxicants to establish the baseline levels in non-vaccinated animals.