Presquevu (from French, meaning “almost seen”) is the sensation of being on the brink of an epiphany. Often very disorienting and distracting, presquevu rarely leads to an actual breakthrough. Frequently, one experiencing presquevu will say that they have something “on the tip of their tongue .”
In life, my focus often becomes searing, too often on folly, or distractions, but on occasions this ”fixation” is a great friend.
One fixation, was how to feed our daughter, once solids started, how to not undo all the strides Arya had made. We failed hopelessly, but Arya knew, she found Olives, she knew what they gave to her, yet her father had studied decades and failed to complete a great picture, until Arya compelled it, then gave it us when we scrambled in our minds dirt.
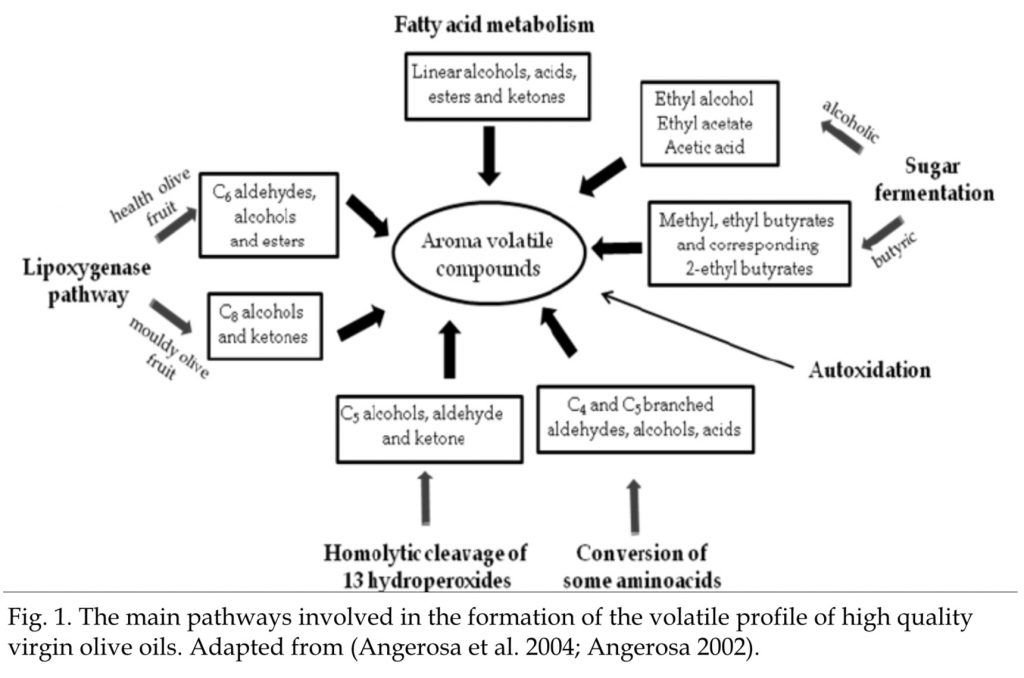
The smell (hexanol) compounds in Olive Oil, are hugely medicinal. The phenolic content is also medicinal, these are crucial factors, in the Liver, Pancreas, Gallbladder, Sphincter all being stimulated to secrete, contract and function (Tryptophan, Cholecystokinin, Serotonin, Insulin et al). An essay on this core bio-chemistry will follow, suffice to say, it’s important and deeply complex stuff, Arya just knew:
Arya, of course, is not spouting the above, she is just feeling her way through things.
This similar theme, of Presque Vu, was found in Arya when we stimulated our friendly bacteria by making Kombucha. After months of this noble adventure, Daddy had become proficient, to the point everybody seemed to like my Kombucha, especially an Organic Apple, Carrot and Ginger second ferment blend.
When trying differing Green Teas, Sencha smooth, delicate. Others like Chun Mee more powerfully effervescent but also more acidic (Sencha for low fizz gently, Chun Mee for high fizz we had mostly settled upon), it was suggested out of the blue by Arya that using Artichoke may yield better results ”Ummm, I think it would be better if you used Artichoke Daddy”.
Daddy, being a man of considerable age and experience, nonchalantly entertained Aryas words, while my Ego dismissed this, as Arya after finding Olives, found Artichokes. So, naturally I listened and reflected that I would research, but was not sure the taste would be what we sought.
Then, to my astonishment (and, I really should have known better, by then), Arya knew this:
Malbaša et al. (2001) used the tubers of composite Jerusalem Artichoke(Helianthus tuberosus L.). They found that the drink obtained could be considered a dietary product because it had a low concentration of sugars after the fermentation process (28 °C/21 days) and the presence of inulo-oligosaccharides.
So, Arya yet again, knew or had the mind to hear, that qualities beyond my fathom, were inherent, in foods she was drawn to.
If experience hadn’t taught me otherwise, it would seem impossible.
The inulo-oligosaccharides, are very powerful sugar feeders of friendly bacteria!!! Our invisible resident, but endangered, Alchemists.
Results: Overall, nine original articles reported the effects of inulin on microbiome composition in adult humans, most of them being randomized, double-blind, placebo-controlled trials (n = 7)… The most consistent change was an increase in Bifidobacterium. Other concordant results included an increase in relative abundance of Anaerostipes, Faecalibacterium, and Lactobacillus, and a decrease in relative abundance of Bacteroides after inulin supplementation.
To note, research is more and more showing, the supplementation of Inulin and/or Pectin has great benefits to out resident Alchemical potency, the younger the person, the stronger or more enduring this recolonisation effect may be (on top of cutting back on processed sugars and oxygen stifling oils).
How was it possible? After researching years, decades, that my 4year old (at that time), knew much, much, better than me?!
Thank heavens she did. Slowly we are catching her up. These days, we share a Kombucha with dinner and a spoonful of Inulin (Cake mix, the girls call it!). Though I never did make the Kombucha with it!
Wenju Lu, Xiaoqing Liu, Tao Wang, Fei Liu, Airu Zhu, and Yongping Lin
Patients with coronavirus disease 2019 (COVID-19) exhibit a spectrum of respiratory symptoms like cough and dyspnea.1–3 Airway mucus is an adhesive viscoelastic gel composed mostly of high-molecular-weight mucous glycoproteins and water, which is important in maintaining lung function and health, pathological mucus hypersecretion may cause airway obstruction and lead to respiratory distress. Mucin (MUC) glycoproteins are the major macromolecular components of mucus, which are classified into two major types: the gel-forming secreted MUC5AC and the membrane-tethered MUC1.4 Here, with an attempt to understand the lung changes, we sought to provide a delineation of the components of airway mucus from patients with COVID-19.
To clean airway obstruction, respiratory tract mucus was aspirated and collected via bronchoscopy from COVID-19 patients with a critical illness, and optical coherence tomography (OCT) was applied via bronchoscopy to obtain cross-sectional images of the bronchiole. For healthy control, sputum was induced by inhaled hypertonic (3%) saline solution delivered with an ultrasonic nebulizer. After collection, sputum was processed as previously described for components analysis.5 Medical history, and clinical and laboratory data of the participants were extracted from electronic medical records. The study was approved by the Ethics Committee of the First Affiliated Hospital of Guangzhou Medical University (No. 2020-65). The requirement for informed consent was waived because the study was observational and the family members were in quarantine.
MUC5AC (sc-21701; Santa Cruz, Shanghai, China) and MUC1 (sc-6827; Santa Cruz) in airway mucus were measured using enzyme-linked immunosorbent assay, and MUC1-cytoplasmic tail (CT, clone EP1024Y; Abcam, Shanghai) levels were measured by Western blot analysis as described previously.5 The levels of MUC5AC and MUC1 were normalized to their average signal reading of a healthy control group.
A total of 16 patients with COVID-19 were included in this study, the clinical characteristics of the recruited subjects were shown in Table S1. There was no significant deviation in the distribution of age, or sex between the cohorts of case and control subjects. All the patients with COVID-19 were admitted to the intensive care unit because of low oxygenation index (199 ± 23 mm Hg), and 79% of them received mechanical ventilation. Blood laboratory tests showed elevated inflammatory indexes including leukocyte count, C-reactive protein, and interleukin-6 in most of the patients with COVID-19 (Table S2).
OCT indicated clear bronchiole in healthy controls (Figure 1A) and mucus retention in the bronchiole of patients with COVID-19 (Figure 1B). A volume of 1-8 mL white to gray sputum with high viscosity (Figure 1C) was aspirated from the respiratory tract of 16 patients with COVID-19. Induced sputum from healthy control was clear and transparent with low viscosity. Compared to healthy control, airway mucus from patients with COVID-19 had a higher level of MUC5AC (Figure 1D), MUC1 (Figure 1E), and MUC1-CT fragment (Figure 1F). However, there were no significant differences in the concentration of total protein, sodium, or chloride in the airway mucus from patients with COVID-19 when compared to healthy control (Table S3).
Representative cross-sectional images of bronchioles in (A) healthy and (B) critical ill COVID-19 patients were obtained with optical coherence tomography and bronchoscopy. C, Airway mucus aspirated by bronchoscopy. D, MUC1 and (E) MUC5AC protein levels as measured by ELISA, and (F) MUC1-CT level as measured by Western blot analysis in the airway mucus from COVID-19 patients and healthy control (HC). The levels of MUC5AC and MUC1 were normalized to their average signal reading of healthy control group. COVID-19, coronavirus disease 2019; CT, cytoplasmic tail; ELISA, enzyme-linked immunosorbent assay; MUC, mucin
Although more than half of patients with COVID-19 presented with a dry cough,6 this study provided direct evidence showing mucus retention in the small airway of patients with COVID-19, and patients were not able to expectorate by themselves and need bronchoscopy aspiration to help them to clean respiratory tract. The sputum from these patients with COVID-19 was viscous, which is not surprising as MUC5AC levels are extremely high, hyperconcentration of this gel-forming MUC dehydrates airway surfaces and causes mucus adhesion, which may contribute to airflow obstruction and respiratory distress. Clearance of airway mucus is an important way to increase oxygen and carbon dioxide exchange, bronchoscopy aspiration of airway mucus was used in all our patients to relieve hypoxia. In our center, all the 16 critical ill COVID-19 patients recovered and were discharged from hospitalization, which may attribute to our aggressive clearance of the respiratory tract. It is of note that bedside bronchoscopy may not be available in some hospitals as the medical resources are limited during the COVID-19 pandemic, carbocisteine has been reported to inhibit airway MUC5AC secretion, which could be used to reduce sputum viscosity and elasticity in patients with COVID-19. In addition, hydration of sputum by aerosolized hypertonic saline solutions or mannitol, and dilation of bronchi via aerosolized salbutamol may facilitate sputum expectoration.
MUC1 is a membrane-tethered MUC expressed on the apical surface of epithelial cells.7, 8 Since MUC1-CT fragment is on the cytoplasmic side of the cells, the elevated sputum CT fragment in patients with COVID-19 could come from detached and disrupted epithelial cells, which is evidenced by the pathological findings of diffuse alveolar damage with fibromyxoid exudates and macrophage infiltration in the lung tissue from patients with COVID-19.9
The limitation of this study is that induced sputum was used in the control group to compare airway mucus aspirated via bronchoscopy from patients with COVID-19, because it was very difficult for the patients with COVID-19 to expectorate sputum even with hypertonic saline solution inhalation.
The findings may suggest that increased level of MUCs in the airway mucus may contribute to the high viscosity of airway mucus and sputum retention in the small airway of patients with COVID-19, airway mucus clearance may be indicated to relieve respiratory distress, and MUC5AC may serve as a target for mucolytic agents in treating COVID-19. And MUC1-CT may serve as an indicator reflecting the severity of airway and alveolar epithelial cell damage.
ACKNOWLEDGMENTS
This study was supported by grants from the National Key R&D Project (2016YFC0903700 and 2016YFC1304102), the National Natural Science Foundation of China (81520108001 and 81770043), and grant specific for COVID-19 study from Guangzhou Institute of Respiratory Health. The authors would like to thank Dr Kwang Chul Kim (University of Arizona) for the invaluable assistance with the manuscript.
CONFLICT OF INTERESTS
The authors declare that there are no conflict of interests.
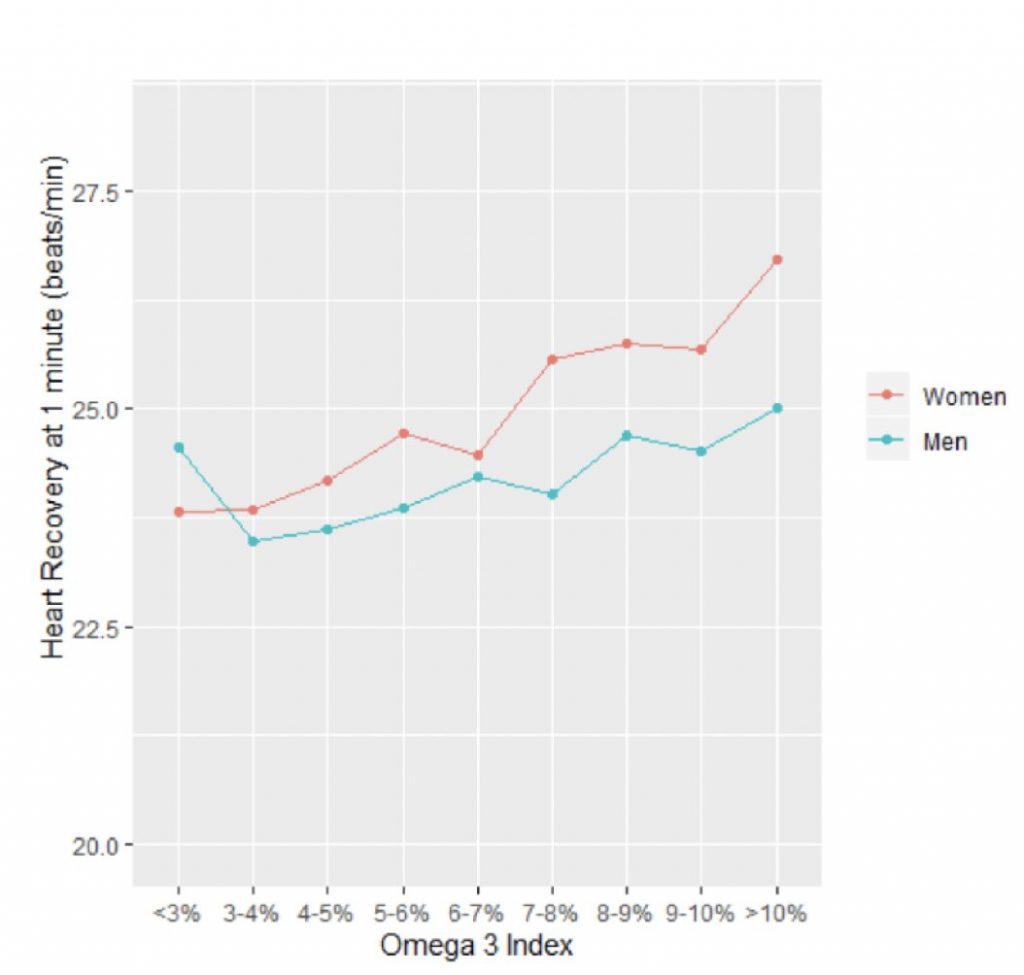
Comparing each patient’s heart rate recovery with their Omega-3 Index, the researchers found a significant relationship between these two variables such that the higher the Index, the faster the heart rate dropped down. The effect was more marked in women than men, but statistically significant in both. This is summarized in Figure 1 (right) where the Omega-3 Index is plotted on the x-axis, and the drop in heart rate one minute after stopping the treadmill test (measured in beats per minute, bpm) is shown as a positive number on the y-axis. Credit: Fatty Acid Research Institute
The Fatty Acid Research Institute (FARI) has published a new research paper in conjunction with The Cooper Institute on omega-3s and heart rate recovery.
Omega-3 fatty acids have a long history of being heart healthy, but exactly why and how has been less clear. They are known to lower serum triglyceride levels, but the effect is relatively small and it’s not clear how much of a risk factor high triglyceride levels is in the first place. So how do the omega-3 fatty acids EPA and DHA work?
A recent study from the Cooper Center Longitudinal Study (CCLS) and FARI sheds new light on this question.
The investigators utilized data from 13,912 healthy men and women who had preventive medical examinations at Cooper Clinic in Dallas over a 10-year period. These examinations routinely included both treadmill exercise testing and measurement of the Omega-3 Index (i.e., red blood cell EPA+DHA levels from OmegaQuant Analytics).
One component of the exercise test is called ‘heart rate recovery’ and it refers to how quickly the heartbeat slows down after maximal exercise. The faster it drops, the healthier the heart.
Comparing each patient’s heart rate recovery with their Omega-3 Index, the researchers found a significant relationship between these two variables such that the higher the Index, the faster the heart rate dropped down. The effect was more marked in women than men, but statistically significant in both. This is summarized in the Figure 1 (right) where the Omega-3 Index is plotted on the x-axis, and the drop in heart rate one minute after stopping the treadmill test (measured in beats per minute, bpm) is shown as a positive number on the y-axis. These are the unadjusted values. (For example, 25 bpm on the y-axis means that 1 minute after stopping exercising—i.e., the maximal heart rate—the person’s heart rate dropped by 25 bpm).
When adjusted for age, maximal METS (a measure of cardiorespiratory fitness), BMI and smoking status, a 2-percentage point higher Omega-3 Index was associated with a 0.35 and 0.69 bpm greater heart rate recovery in men and women, respectively (p<0.001 both).
Previous studies have shown that a slow heart rate recovery is associated with increased risk for sudden cardiac death, which fits with higher EPA and DHA levels being linked with reduced risk for sudden cardiac death3.
Dr. William Harris, President of FARI and co-inventor of the Omega-3 Index, who was also an author on the study, commented on the implications of this research. “These new findings from the CCLS harmonize with the known benefits of omega-3 fatty acids on resting heart rate and provide new clues to how these important fatty acids can preserve cardiac health,” he said.
“These benefits on cardiac autonomic tone join other cardioprotective effects of omega-3 fatty acids, including the reduction in blood pressure, chronic inflammation and platelet aggregation, to at least partially explain why omega-3s are good for the heart. Future treatment studies should define the omega-3 intake (and Omega-3 Index) that optimizes this aspect of cardiac function.”
Dr. James H O’Keefe, MD, a cardiologist and Medical Director of the Charles and Barbara Duboc Cardio Health & Wellness Center at Saint Luke’s Mid America Heart
Institute in Kansas City, MO, and a Professor of Medicine at the University of Missouri-Kansas City (who was not involved with the study) remarked that this research provides “strong data supporting the robust cardiovascular benefits of omega-3 fatty acids.”
The health effects of omega-3 fatty acids have been controversial. Here we report the results of a de novo pooled analysis conducted with data from 17 prospective cohort studies examining the associations between blood omega-3 fatty acid levels and risk for all-cause mortality. Over a median of 16 years of follow-up, 15,720 deaths occurred among 42,466 individuals. We found that, after multivariable adjustment for relevant risk factors, risk for death from all causes was significantly lower (by 15–18%, at least p < 0.003) in the highest vs the lowest quintile for circulating long chain (20–22 carbon) omega-3 fatty acids (eicosapentaenoic, docosapentaenoic, and docosahexaenoic acids). Similar relationships were seen for death from cardiovascular disease, cancer and other causes. No associations were seen with the 18-carbon omega-3, alpha-linolenic acid. These findings suggest that higher circulating levels of marine n-3 PUFA are associated with a lower risk of premature death.
Introduction
The n-3 polyunsaturated fatty acid (PUFA) family has been the subject of intense investigation ever since their inverse associations with risk for acute myocardial infarction were reported in Greenland Eskimos in the 1970s1,2. The PUFAs in this family include the 18-carbon, plant-derived alpha-linolenic acid (ALA,) as well as the 20–22-carbon, long-chain (LC, mostly seafood-derived) eicosapentaenoic (EPA), docosapentaenoic (DPA), and docosahexaenoic (DHA) acids.
The efficacy of the LC n-3 PUFAs in reducing risk for cardiovascular disease (CVD) remains controversial as findings from different randomized controlled trials (RCTs) have been conflicting. Nevertheless, a 2019 meta-analysis of RCTs reported significant reductions in risk for myocardial infarction, coronary heart disease (CHD) events and mortality, and CVD mortality in patients randomized to supplemental LC n-3 PUFAs3. Another meta-analysis of observational studies found that higher levels of circulating LC n-3 PUFA levels were significantly associated with a lower risk for CHD death4. However, no meta-analysis has yet examined the relationship between LC n-3 PUFAs blood levels and risk for all-cause mortality. Indeed, the only meta-analyses to report a beneficial association with all-cause mortality were based on the self-reported intake of fish5,6. Fish contain many nutrients besides just LC n-3 PUFAs, self-reported food intake is memory dependent, food databases can be out of date, and fish meals often replace less healthful choices. As a result, studies that link LC n-3 PUFAs and health outcomes based on self-reported fish intake have potential limitations. A more reliable and objective measure of LC n-3 PUFA consumption is their level in the blood7 which is primarily determined by the consumption of preformed LC n-3 PUFAs (although synthesis from dietary ALA can make a small contribution8). Hence a clearer picture of the biological relationship between LC n-3 PUFAs and disease outcomes may be obtained from biomarker-based investigations.
Some studies have reported inverse relations between n-3 PUFA biomarkers and total mortality9,10,11, while others have not12,13. In the Cardiovascular Health Study, higher LC n-3 PUFA levels also were associated with overall “healthier aging” (i.e., surviving past age 65 free of chronic diseases and maintaining good functional status)14. However, reports from studies of individual cohorts can be limited by insufficient power and inconsistent adjustment for potential confounding factors. In addition, publication bias can distort summary conclusions. To address these challenges, the present study pooled de novo individual-level analyses across 17 prospective cohort studies in the Fatty Acid and Outcome Research Consortium (FORCE)15 to explore the associations of circulating levels of n-3 PUFAs (both plant- and seafood-derived) and all-cause mortality. Secondarily, we examined the associations with mortality from CVD, cancer, and all other causes.
Here, we show significant inverse associations for all mortality endpoints with the LC n-3 PUFA levels. Hence, chronically higher tissue levels of these FAs operating through a variety of potential mechanisms may slow the aging process.
Results
Population
The pooled analyses included circulating n-3 PUFA measurements on 42,466 individuals, 15,720 (37%) of whom died during follow-up (Table 1). At baseline, the average age was 65 years (range of mean ages across cohorts was 50–81 years), 55% were women (range of 0–100% across cohorts) and the median follow-up time was 16 years (range of 5–32 years across cohorts). Whites constituted 87% of the sample. Circulating levels of the n-3 PUFAs (and of the n-6 PUFAs linoleic and arachidonic acids, which were included as covariates) are shown in Supplementary Fig. 1 and in Supplementary Table 2. Supplementary Table 3 shows the number of cause-specific deaths from participating cohorts. Overall, approximately 30% of the deaths were attributed to CVD, 30% to cancer, and the remaining 39% to all other causes.
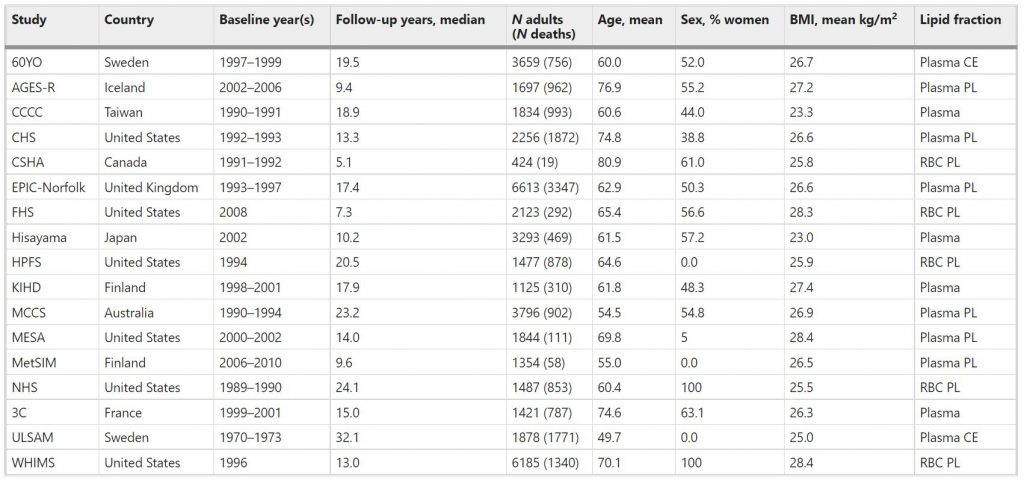
Table 1 Baseline characteristicsa of 17 prospective cohort studies included in the meta-analysis: Fatty Acids and Outcomes Research Consortium.
aBaseline characteristics at the time of fatty acid biomarker measurement. Abbreviations of cohorts: 60YO, Stockholm cohort of 60-year olds, AGES-R Age, Genes, Environment Susceptibility Study (Reykjavik), CCCC Chin-Shan Community Cardiovascular Cohort Study, CHS Cardiovascular Health Study, CSHA Canadian Study of Health and Aging, EPIC-Norfolk European Prospective Investigation into Cancer, Norfolk UK, FHS Framingham Heart Study, HPFS Health Professionals Follow-up Study, KIHD Kuopio Ischemic Heart Disease Risk Factor Study, MCCS Melbourne Collaborative Cohort Study, MESA Multi-Ethnic Study of Atherosclerosis, MetSIM Metabolic Syndrome in Men Study, NHS Nurses’ Health Study, 3C Three-City Study, ULSAM Uppsala Longitudinal Study of Adult Men, WHIMS Women’s Health Initiative Memory Study. CE cholesteryl esters, PL phospholipids, RBC red blood cells.
Total mortality
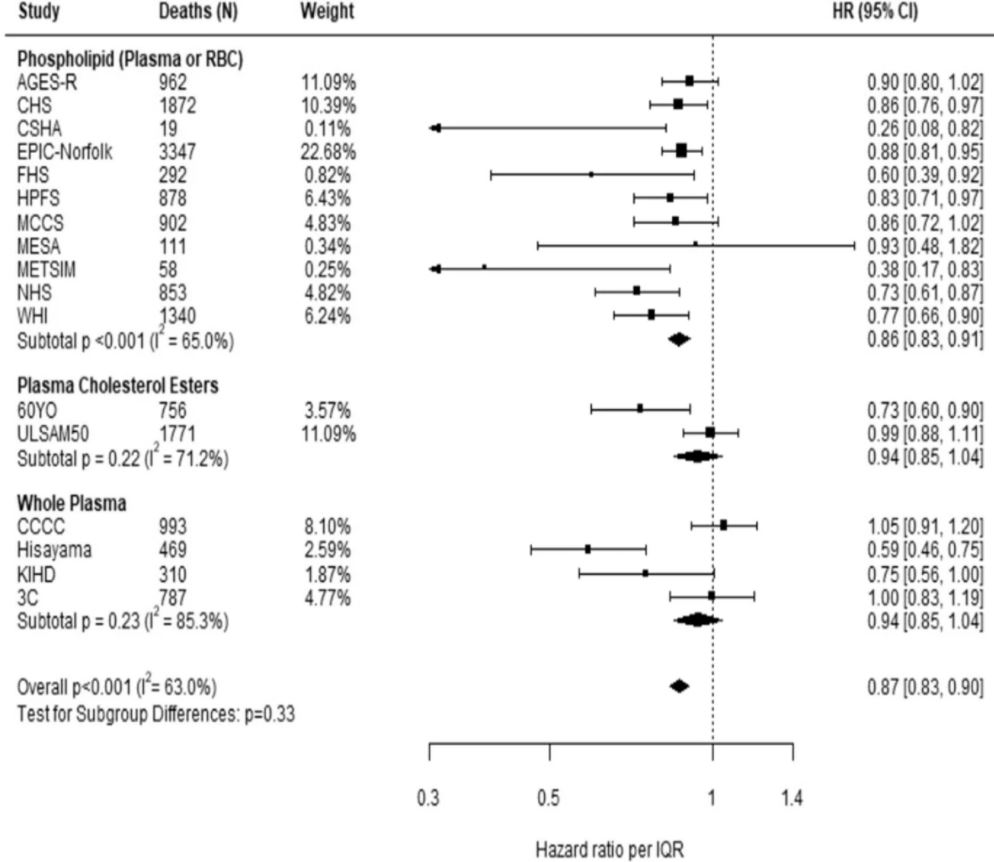
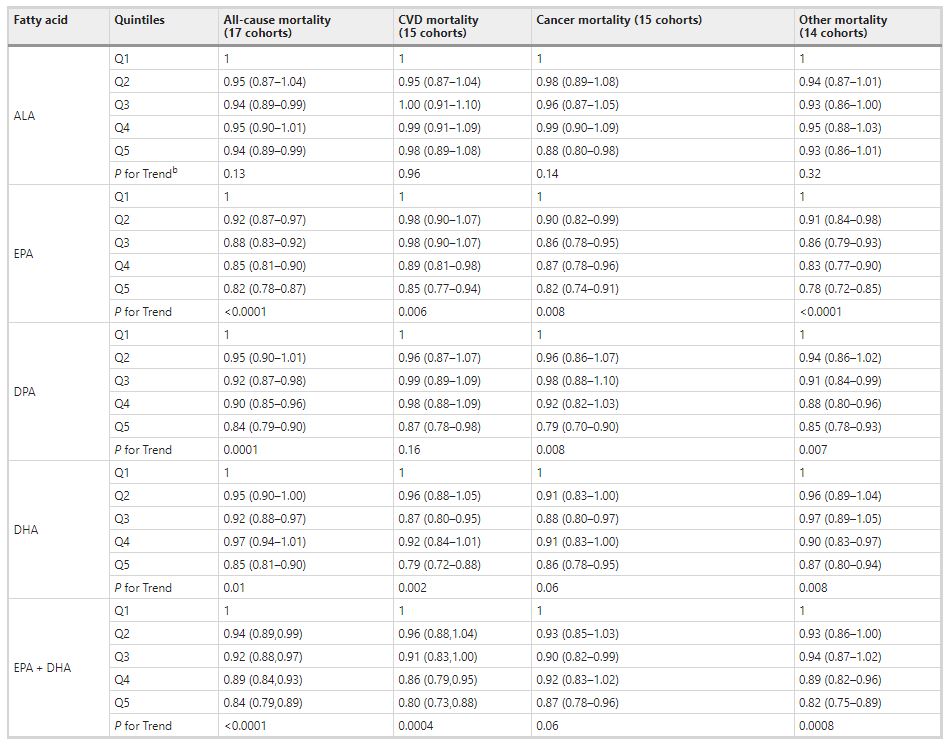
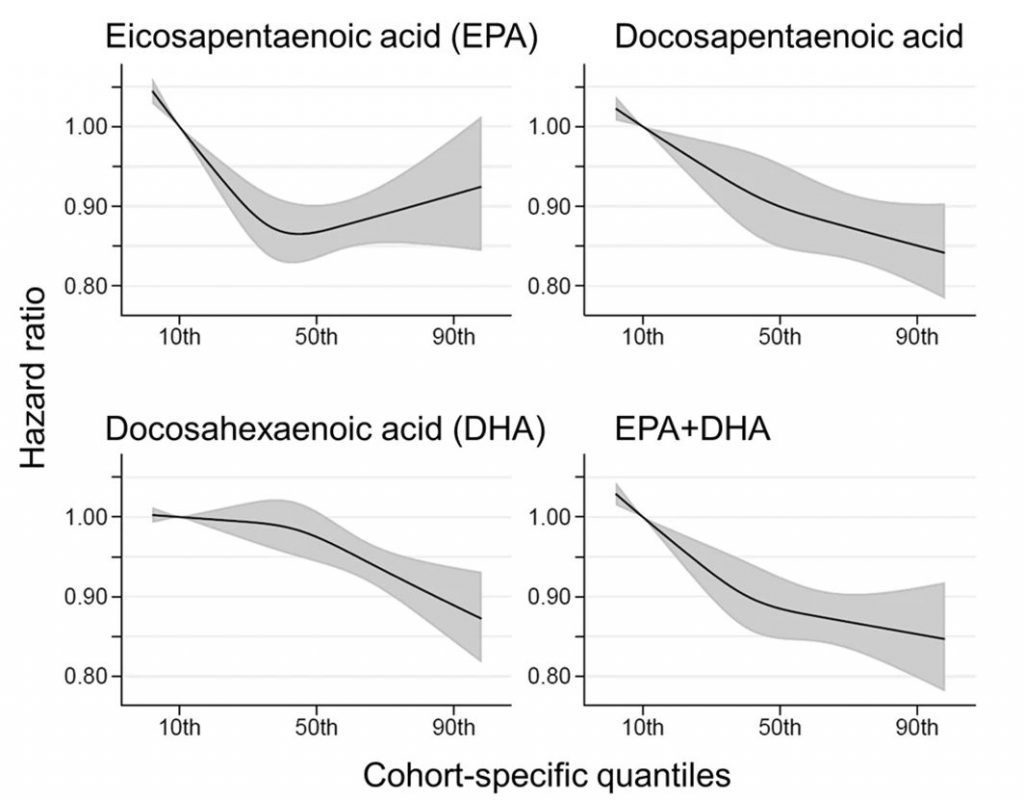
Comparing the medians of the first and fifth quintiles (i.e., approximately the 90th and the 10th percentiles), higher EPA, DPA, DHA, and EPA + DHA levels were associated with between 9% and 13% lower risk of all-cause mortality (Table 2). (The fatty acid levels associated with these percentiles for each cohort and sample type are shown in Supplementary Table 4). The HR for total mortality for EPA + DHA was 0.87 (95% CI: 0.83–0.90) (Fig. 1). In contrast, ALA was not significantly associated with all-cause mortality [HR 0.99 (0.96–1.02)]. In an across quintiles analysis, significant trends were observed for EPA, DPA, DHA, and EPA + DHA (all < 0.01); and comparing the top to the bottom quintile, each was associated with 15–18% lower risk of death (Table 3). There was little evidence for nonlinearity in these inverse associations for all each LC n-3 PUFAs except for EPA (p = 0.002 for the nonlinearity; Fig. 2). The relationship of EPA with mortality was most pronounced at lower levels and then appeared to plateau at higher levels. ALA was generally unassociated with total mortality, except for a borderline association in the top quintile [HR 0.94 (0.89–0.99); P-trend = 0.13], and there was no evidence for nonlinearity (Supplementary Fig. 2).
Hazard ratios (HRs) and 95% CIs expressed per cohort-specific inter-quintiles range comparing the midpoint of the top and bottom quintiles (see Supplementary Table 4 for cohort-specific n-3 PUFA values). All HRs are adjusted for age, sex, race, field center, body-mass index, education, occupation, marital status, smoking, physical activity, alcohol intake, prevalent diabetes, hypertension, and dyslipidemia, self-reported general health, and the sum of circulating n-6 PUFA (linoleic plus arachidonic acids). See Supplementary Table 4 for the 10th and 90th percentile values from each cohort for each PUFA of interest and the average PUFA values per lipid pool. Abbreviations: ALA alpha-linolenic acid, CI confidence interval, CVD cardiovascular disease, DHA docosahexaenoic acid, DPA docosapentaenoic acid, EPA eicosapentaenoic acid, HR hazard ratio.
Fig. 1: Adjusted hazard ratios (HR, 95% CI) for total mortality for circulating eicosapentaenoic (EPA) plus docosahexaenoic acid (DHA) in the 17 contributing studies of the Fatty Acids and Outcomes Research Consortium.
Study-specific estimates for HRs (dark squares) are shown per interquartile range (comparing the midpoint of the top to the bottom quintiles) their sizes indicate study weights (column 3). The horizontal line through each HR is 95% CI. Compartments included erythrocyte phospholipids, plasma phospholipids, cholesteryl esters, and total plasma. All HRs are adjusted for age, sex, race, field center, body-mass index, education, occupation, marital status, smoking, physical activity, alcohol intake, prevalent diabetes, hypertension, and dyslipidemia, self-reported general health, and the sum of circulating n-6 PUFA (linoleic plus arachidonic acids). See Table 1 footnote for abbreviations of cohorts.
Table 3 Meta-analysis of circulating n-3 PUFA biomarkers with mortality types by cohort-specific quintiles (hazard ratios and 95% CIsa): Fatty Acids and Outcomes Research Consortium.aExpressed per cohort-specific quintiles (see Supplementary Table 4 for cohort-specific n-3 PUFA values). All hazard ratios are adjusted for age, sex, race, field center, body-mass index, education, occupation, marital status, smoking, physical activity, alcohol intake, prevalent diabetes, hypertension, and dyslipidemia, self-reported general health, and the sum of circulating n-6 PUFA (linoleic plus arachidonic acids). bP-for trend is computed by using a fixed-effects, inverse weighted meta-regression analysis, i.e., the hazard estimates were regressed against study quintiles, which we assigned a value of 1, 2, 3, 4, or 5. Abbreviations: ALA alpha-linolenic acid, CI confidence interval, CVD cardiovascular disease, DHA docosahexaenoic acid, DPA docosapentaenoic acid, EPA eicosapentaenoic acid.
Fig. 2: Associations of circulating long-chain n-3 PUFA levels with all-cause mortality: nonlinear dose-response meta-analysis in the Fatty Acids and Outcomes Research Consortium. Hazard ratios and cohort-specific quantiles are presented in the vertical and horizontal axis, respectively.
The best estimates and their confidence intervals are presented as black lines and gray-shaded areas, respectively. The 10th percentile was selected as a reference level and the x-axis depicts 5th to 95th percentiles. Potential nonlinearity was identified for EPA (p = 0.0004) but not for the others (p > 0.05). All HRs are adjusted for age, sex, race, field center, body-mass index, education, occupation, marital status, smoking, physical activity, alcohol intake, prevalent diabetes, hypertension, and dyslipidemia, self-reported general health, and the sum of circulating n-6 PUFA (linoleic plus arachidonic acids).
Cause-specific mortality
Comparing the 90th to the 10th percentile, each of the LCn-3 PUFAs was significantly associated with a lower risk for death from CVD, cancer, and all other causes combined [except for DHA and cancer mortality, HR 0.93 (0.86–1.00)] (Table 2). ALA was not significantly associated with any cause-specific mortality. Evaluating the trend across quintiles, EPA, DHA, and EPA + DHA were inversely associated with CVD death, EPA and DPA were inversely associated with cancer death, and each of the LC n-3 PUFAs was inversely associated with other death. Comparing the top to the bottom quintile, EPA, DPA, DHA, and EPA + DHA were each significantly, inversely associated with CVD, cancer, and other mortality (Table 3).
Heterogeneity and sensitivity analyses
Inter-cohort heterogeneity was at least moderate (I2 > 50%) in the pooled analyses of all-cause mortality for all n-3 PUFAs except ALA (I2 = 26%) and EPA (I2 = 41%), while heterogeneity for cause-specific mortality ranged from little to moderate (0–56%) (Supplementary Table 5). There was little evidence of differential associations with mortality by PUFA lipid compartment after accounting for multiple testing (5 PUFAs × 4 outcomes; Bonferroni correction 0.05/20 = 0.0025, Supplementary Table 6). Likewise, associations of n-3 PUFAs with total mortality were similar across strata based on age, sex, race, and fish oil use (Supplementary Table 7), with no significant differences after accounting for multiple testing (5 PUFAs × 4 strata results; Bonferroni correction 0.05/20 = 0.0025). Overall findings did not change with the removal of participants taking fish oil (Supplementary Table 7) or in the drop-one-cohort analyses.
Discussion
In this meta-analysis utilizing a harmonized analytical strategy with individual-level data from 17 cohorts, we examined the associations between circulating levels of the n-3 PUFAs and mortality. We found that, after controlling for other major risk factors, LC n-3 PUFAs (but not ALA) were associated with about a 15–18% lower risk of total mortality comparing the top to the bottom quintiles. These relationships were generally linear for DPA, DHA, and EPA + DHA, but not for EPA. For this PUFA there was a steeper risk reduction across the lower blood levels but little additional difference in risk at higher blood levels. Inverse correlations were also generally observed between LC n-3 PUFA levels and CVD, cancer, and other causes of death.
This pooled analysis including over 40,000 participants and over 15,000 deaths greatly expands upon the findings of prior individual cohort studies that examined associations of circulating levels of n-3 PUFAs and all-cause mortality9,10,11,12,13,16,17,18,19,20,21,22,23,24. Relatively few studies have evaluated self-reported dietary fish (or estimated n-3 PUFA) intake in relation to total mortality, but those that have typically support our observations here5,22,25,26. Interestingly, reported use of fish oil supplements was linked to a lower risk for death from any cause in a study from the UK including over 427,000 individuals27.
Associations with total and cause-specific mortality were not significant for the plant-derived n-3 PUFA ALA. Prior biomarker-based meta-analyses reported inverse associations of ALA with CHD death, but relationships with total or CVD mortality were not examined4,28. Whether our finding of no association ALA on CVD mortality was because ALA has no role to play in fatal strokes (included in the CVD mortality metric) or because of differences in the cohorts included in these prior meta-analyses vs. the present one is not clear. Circulating ALA levels are less dependable markers of intake compared with the LC n-3 PUFAs because this fatty acid is rapidly β-oxidized and, to a small extent, converted into the LC n-3 PUFAs8. Nevertheless, the borderline and inconsistent relations of ALA on mortality risk deserve further study.
Higher circulating levels of LC n-3 PUFAs may beneficially affect diverse cellular systems that together could contribute to a reduced risk for death. The mechanisms behind the ostensibly beneficial effect of LC n-3 PUFAs on human biology are multiple and have been summarized in several recent reviews papers29,30,31,32. Among them are hypotriglyceridemic, antihypertensive, and antiplatelet effects; as well as positive effects on adipocyte biology, endothelial function, and autonomic balance. All of these appear to be mediated by effects on membrane physiochemistry, gene expression, and the production of a myriad of bioactive oxylipins. Persistently lower levels of inflammatory biomarkers also characterize those with higher circulating LC n-3 PUFA levels33. These fatty acids have been reported to inhibit the mammalian (or mechanistic) target of rapamycin (mTOR) in animal studies showing benefits in cancer34, metabolic syndrome35, spinal cord injury36, and depression37. mTOR inhibition extends lifespan in many species38 and acts as an energy sensor to coordinate gene expression, ribosome biogenesis, and mitochondrial metabolism39. In the Heart and Soul Study, where whole blood EPA + DHA levels were inversely associated with all-cause mortality24, higher levels were also linked with a slower rate of telomere shortening over a 5-year period40. As higher rates of telomere attrition have been associated with shorter overall lifespan41,42, this finding may be secondary to the more distal biochemical mechanisms noted above. Regardless of their specific actions, higher cellular levels of the LC n-3 PUFAs appear to slow the aging process.
Our findings of lower risk of CVD death with high vs. low blood levels of EPA + DHA are generally consistent with meta-analyses of self-reported fish intake25 and of biomarker levels4, as well as randomized controlled clinical trials of n-3 PUFA supplementation3,43 (although the most recent trial44 has not yet been included in meta-analyses). Compared with CVD, evidence for a link between n-3 PUFAs and cancer mortality risk is sparse, with no significant relationship for self-reported estimates of fish or n-3 PUFA consumption25,45. Meta-analyses of RCTs with n-3 PUFA supplements also have not observed effects on cancer, although short-term durations of such trials (generally up to 5 years) would likely preclude any ability to detect an effect on cancer46,47. The difference between these findings and what we observed may arise from the use of biomarker levels instead of self-reported fish intake. Biomarkers are potentially truer reflections of long-term exposure, making it easier to detect subtle relationships. In addition, circulating LC n-3 PUFA levels reflect endogenous metabolism, especially for DPA which is not correlated with estimated dietary DPA intake48 but may have important biologic effects49. Finally, since neurodegenerative diseases are a major non-CVD, non-cancer cause of death, a report that higher fish intake was associated with reduced mortality from this cause6 is consistent with our observations here.
Although circulating marine n-3 PUFA levels have not been measured in all of the major intervention trials, the doses of EPA + DHA used in most trials (<1 g/day) may not have resulted in marked differences in levels between treated and control patients50. For example, in the Vitamin D and Omega-3 Trial (VITAL) trial, treatment with 840 mg of EPA + DHA per day increased plasma phospholipid EPA + DHA levels from 2.7 to 4.1%, a 55% increase. This relatively small difference in LC n-3 PUFA levels between the placebo and active treatment groups could be one of the potential reasons for the failure of some RCTs to detect an effect of n-3 PUFAs on CV outcomes50,51. Future RCTs may be more effective if they focus on people with low baseline levels of LC n-3 PUFAs52 and provide doses of EPA and DHA that produce higher blood levels. An intake of about 250 mg of EPA + DHA per day as recommended in the Dietary Guidelines for Americans53 may raise circulating levels into the ranges observed here for some but not all adults7.
Although a significant effect on the primary (composite) endpoint in the VITAL trial47 was not achieved, our findings comport well with some of its secondary findings. In this study, the provision of 840 mg of EPA + DHA/day significantly reduced risk for major CV events and myocardial infarction in those participants with lower (vs. higher) intakes of fish (blood levels in these groups were not reported). There was a significant interaction of fish intake on total mortality as well; the HR (95% CI) in the low intake group was 0.87 (0.73–1.04) and in the high intake group, 1.19 (0.99–1.44, p for interaction 0.017). This secondary observation in VITAL implies that individuals with lower baseline LC n-3 PUFA levels are more likely to benefit from increased levels than those with higher baseline levels. Two recent RCTs examining the effects of high dose (~3–4 g/day) of LC n-3 PUFAs were performed in overweight patients with high blood triglyceride levels and at high risk for CVD events, all on background statin therapy. After 5 years of treatment, Bhatt et al.54 reported beneficial effects of EPA ethyl esters on CV events, whereas Nicholls et al.44 found no effect on the primary outcome using an EPA + DHA product in which the fatty acids were non-esterified. Another 2-year trial in elderly post-MI patients from Norway given 1.8 g of EPA + DHA found no benefit on CV outcomes55. None of these trials is directly relevant to our findings here owing to the nature of the high-risk patient populations, the number of concurrent background medications, the short duration of treatment, and the initiation of treatment late in life.
Strengths of the current analysis include the use of objective n-3 PUFA biomarkers (instead of estimated intakes from dietary questionnaires) which increases the accuracy of exposure assessment and allows for separate analysis of different individual n-3 PUFAs. The use of prespecified, harmonized, de novo individual-level analyses across multiple cohorts substantially increase generalizability, reduces confounding through consistent adjustment for covariates, and limits the potential for publication bias. The pooling of 17 studies including over 15,000 deaths also increased the statistical power to evaluate mortality subtypes as well as potential heterogeneity across subgroups.
Potential limitations deserve attention. Because our outcome was not rare, the hazard ratios (HRs) reported here (instantaneous relative risk) may be modestly different than the cumulative relative risk. Most individuals were White, potentially lowering generalizability to other races/ethnicities, although our analysis still included nearly 6000 non-Whites in whom findings for EPA + DHA were generally similar to those for Whites (Supplementary Table 7). Despite extensive efforts to harmonize study-specific methods, moderate heterogeneity remained between studies that may be due to unmeasured background population characteristics, differences in laboratory assessment of PUFAs and of outcomes, chance, or any combination of these. PUFAs and covariates were measured once at baseline, and changes over time could lead to misclassification, which could bias the results in uncertain directions. On the other hand, reasonable reproducibility has been reported for n-3 PUFA biomarker concentrations over time56. Because analytical methods, even within the same lipid fraction, were not standardized, and n-3 PUFA levels were measured in multiple fractions, we assessed cohort-specific n-3 PUFA percentiles rather than absolute percentages of total fatty acids in each fraction. Since FA levels were reported as a percent of total FAs in each lipid compartment, levels of one FA could affect levels of another. Indeed, in the plasma or RBC PL and CE pools, higher levels of the LC n-3 PUFAs (which were the focus of this study) are linked with lower levels of the n-6 PUFAs but not of saturated or mono-unsaturated FAs57,58. Since we adjusted for differences in linoleic and arachidonic levels in our analyses, this concern was accounted for. Each lipid pool used in this study reflects LC n-3 PUFA intake during relatively different and overlapping time periods generally from months to weeks following this hierarchy: RBC ≥ Plasma PL ≈ Plasma CE ≥ total plasma59,60. In addition, we cannot rule out the potential for residual confounding. That is, higher LC n-3 PUFA levels may simply be markers of a “healthy lifestyle,” and the fatty acids themselves may not be playing any physiological role in postponing death but would be biomarkers of a suite of other healthy behaviors (dietary/exercise/non-smoking, etc.), or endogenous metabolic processes, that might, in a multiplicity of ways, manifest in greater longevity. Although we adjusted for many major risk factors (age, income, marital status, smoking, hyperlipidemia, hypertension, etc.), residual confounding by other factors is always possible. However, the magnitude of the observed effect of the meta-analysis of circulating LC n-3 PUFAs and total mortality reported herein is consistent with the known associations with CHD mortality and sudden cardiac death61,62. Finally, as the attribution of cause of death is never as unambiguous as death itself, some uncertainty must attend to the cause-specific analyses reported here. In summary, in a global pooled analysis of prospective studies, LC n-3 PUFA levels were inversely associated with risk for death from all causes and from CVD, cancer, and other causes.
ChooseLife Notes : None of these studies, on ALA, will have included 37g odd emulsified 18-chain ALA daily, as Budwig studied and found to be the chief propellant to regain electron conductance within the cells. So whilst I like these studies they are biased towards Murine sources unjustly IMO, Flax has the highest level of surplus Electrons, or Pi Electrons, most enriching to our Electron Cloud, as Budwig variously described.
Donald Hathaway III, Krunal Pandav, Madhusudan Patel, Adrian Riva-Moscoso, Bishnu Mohan Singh, Aayushi Patel, Zar Chi Min, Sarabjot Singh-Makkar, Muhammad Khawar Sana, Rafael Sanchez-Dopazo, Rockeven Desir, Michael Maher Mourad Fahem, Susan Manella, Ivan Rodriguez, Alina Alvarez and Rafael Abreu
Corresponding Author: Donald Hathaway III, BSc. Division of Research & Academic Affairs, Larkin Health System, 7031 SW 62nd Avenue, South Miami, FL 33143, USA. Email: donald.hathawayiii@gmail.com
Infect Chemother. 2020 Dec
Abstract
The rapid international spread of severe acute respiratory syndrome coronavirus 2 responsible for coronavirus disease 2019 (COVID-19) has posed a global health emergency in 2020. It has affected over 52 million people and led to over 1.29 million deaths worldwide, as of November 13th, 2020. Patients diagnosed with COVID-19 present with symptoms ranging from none to severe and include fever, shortness of breath, dry cough, anosmia, and gastrointestinal abnormalities. Severe complications are largely due to overdrive of the host immune system leading to “cytokine storm”. This results in disseminated intravascular coagulation, acute respiratory distress syndrome, multiple organ dysfunction syndrome, and death. Due to its highly infectious nature and concerning mortality rate, every effort has been focused on prevention and creating new medications or repurposing old treatment options to ameliorate the suffering of COVID-19 patients including the immune dysregulation. Omega-3 fatty acids are known to be incorporated throughout the body into the bi-phospholipid layer of the cell membrane leading to the production of less pro-inflammatory mediators compared to other fatty acids that are more prevalent in the Western diet. In this article, the benefits of omega-3 fatty acids, especially eicosapentaenoic acid and docosahexaenoic acid, including their anti-inflammatory, immunomodulating, and possible antiviral effects have been discussed.
Introduction
The coronavirus disease 2019 (COVID-19), now known the world over, is an emerging respiratory disease that was first identified in December 2019, in Wuhan, the capital of China’s Hubei province. It has since spread globally, resulting in the ongoing COVID-19 pandemic [1, 2]. In December 2019, this world-changing phenomenon began with an outbreak of pneumonia due to an unknown cause in Wuhan, with an epidemiological link to the Huanan Seafood Wholesale Market Place. The World Health Organization (WHO) was notified on December 31, 2019, by the Chinese Health Authorities [1]. The Chinese Center for Disease Control and Prevention identified a novel coronavirus on January 7, 2020, from the throat swab of a patient, which the WHO subsequently named 2019-nCoV [3]. This respiratory disease rapidly spread beyond the borders of China and by February 15, 2020, 26 countries were affected by this disease [4]. Considering this, the WHO declared it a public health emergency of international concern on January 30, 2020 and called for collaborative efforts of all countries to prevent the rapid spread of the virus [5]. Despite these efforts, the virus continued to spread, and the WHO declared it a pandemic on March 11, 2020 [2]. From its first outbreak in Wuhan, through November 13th, 2020, a total of over 52 million laboratory-confirmed cases of COVID-19 along with over 1.29 million associated deaths, have been reported globally [6]. In the United States (US), the total confirmed cases of COVID-19 have surpassed 10 million with over 240,000 deaths as of November 13th, 2020 [6].
The novel COVID-19 infection in humans may cause a wide range of symptoms, while some patients may remain asymptomatic even if they test positive for the virus. Possible clinical presentations may include fever, fatigue, sore throat, dry cough, shortness of breath, body aches, nasal congestion, anosmia, abdominal pain, and diarrhea, but other less common presentations have been reported as well. The minority of patients may however develop severe symptoms and serious complications such as interstitial pneumonia, septic shock, adult respiratory distress syndrome (ARDS), stroke, disseminated intravascular coagulation (DIC), and multi-organ failure (MODS). Strikingly, even asymptomatic patients are believed to be able to spread the disease [7].
Omega-3 fatty acids (FAs) are polyunsaturated fatty acids (PUFAs) that are abundantly available in nature. Omega-3 FAs belong to a category of supplements known as GRAS (generally recognized as safe). The Omega-3 Index Test serves as a measure of the amount of Eicosapentaenoic Acid (EPA) and Docosahexaenoic Acid (DHA) in the blood, especially in the red blood cell membranes. This index shows the ratio of omega-3 FAs to all other fatty acids. A recent study showed that more than 90% of American people consumed less than the recommended optimal value for omega-3 FAs in the diet (0.17 g/day) [8]. The metabolites of both omega-3 and omega-6 play an important role in the synthesis of different inflammatory mediators such as prostaglandins (PG), leukotrienes (LT), thromboxanes (TX), protectins, and resolvins. Omega-3 FA (fatty acid) plays a role in the host cellular membrane which regulates membrane fluidity and intricate lipid raft assembling in the cell membrane. A study conducted by Gutierrez and colleagues showed that omega-3 FA is incorporated throughout the body into the bi-phospholipid layer of the cell membrane of neutrophils and produces different mediators such as prostaglandins, leukotrienes, and maresins [9]. For that reason, if the injury occurs the byproducts of those cell membranes may produce less inflammatory provoking mediators compared to omega-6, which is more prevalent in the American diet [10]. Omega-3 FAs improve the function of the macrophages by secreting cytokines and chemokines, promoting the ability of phagocytosis, and activating macrophages by polarization [11]. Omega-3 FAs are also known to down-regulate Nuclear Factor-κ Beta (NF-κB). NF-κB is considered to be a transcription factor involved in cell signaling to initiate an inflammatory response by the innate immune system. The study shows that fish oil enhances antiviral response by inducing interferon (IFN) which inhibits viral replication [11]. Omega-3 FAs weaken the antiviral response of CD8 T cells and thereby could potentially be used to modulate cytokine responses to viral invaders [12].
A lack of omega-3 FAs in the diet can change the composition of the cell membrane. Every cell needs a healthy, functioning lipid bilayer to facilitate physiological responses and to maintain fluidity. However, the American diet contains high levels of omega-6 FAs as opposed to omega-3. One of the major causes of death in patients infected with severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) is multiorgan failure, which is a result of immune system overdrive causing cytokine storms. The omega-3 FA is known to produce less pro-inflammatory cytokines, therefore increasing omega-3 FA intake in the diet or supplementation could decrease viral entry, promote better immune function, and decrease severity among those who have been diagnosed with COVID-19. As we are still searching for definitive treatment, omega-3 FAs might be a safe and relatively inexpensive prophylactic and treatment approach for those who are at high risk and those who have the disease. This review aims at describing the health benefits of consuming a diet rich in omega-3 FAs in addition to the possible role in COVID-19.
Coronavirus in Humans
Coronaviruses are a family of spherical viruses, and their surfaces are covered with ‘crown-like’ spikes. These viruses are enveloped with single-stranded linear positive-sense RNA genomes. They are classified under the order Nidovirales, family Coronaviridae, and subfamily Orthocoronavirinae [13]. They have the largest genome for RNA viruses and based on genetic and antigenic criteria, they have been divided into four genera: alpha, beta, gamma, and delta Coronaviruses [14]. They have been widely distributed in nature and can affect other species like birds, bats, cats, rodents, pigs, and other mammals [15]. The seven coronaviruses that infect humans are SARS-CoV-2, alphacoronavirus 229E and NL63, and betacoronavirus HKU1, OC43, coronavirus associated with the SARS-CoV and coronavirus associated with respiratory syndrome in the Middle East (MERS -CoV) [16].
A wide range of similarities exists between SARS-CoV and SARS-CoV-2, as shown in Table 1. Both of them belong to the family Coronaviridae [17]. Studies show that there is a 76.47% similarity in amino acid sequences in both of them [18]. Comparison of RNA sequence and protein modeling showed that the domain on the spike protein which is responsible for attaching SARS-CoV-2 to the receptors on the host cell is similar to SARS-CoV [19]. Both use angiotensin-converting enzyme 2 (ACE-2) receptors for entry in the human respiratory epithelium cells [5, 17]. They are transmitted by respiratory droplets and contact with infected people [20, 21] and responsible for causing symptoms like fever, cough, shortness of breath, and fatigue [22]. They cause the appearance of ground-glass opacities on the Chest X-ray. The simple way to prevent them is by hand hygiene, social distancing, and respiratory hygiene [21]. MERS-CoV uses Dipeptidyl peptidase-4 (DPP4), CD26 receptors to attach to the respiratory epithelial cells, and pneumocytes [17].
SARS-CoV, severe acute respiratory syndrome coronavirus; MERS-CoV, Middle East respiratory syndrome coronavirus; SARS-CoV-2, severe acute respiratory syndrome coronavirus-2; N/A, not applicable; ACE-2, angiotensin-converting enzyme 2; DPP4, dipeptidyl peptidase 4; CD26, cluster of differentiation 26.
The basic reproduction number (R0) of COVID-19 is between 1.4 to 2.5 according to the statement based on January 23rd, 2020. R0 is much higher for COVID-19 compared to that of SARS (1.7 – 1.0) and that of MERS (<1). COVID-19 has been a clinical mystery, as of now, with unique epidemiology, pathogenesis, and clinical outcomes [23]. This type of attachment enhances viral fusion to the human cells and atypical severe clinical outcomes in the host. ACE-2 receptors are present in the heart, lungs, gastrointestinal tract, and blood vessels. ACE-2 receptors are the receptors that mediate the viral entry of SARS-CoV-2, causing vasoconstriction, inflammation, and thrombosis [17, 24].
The diameter of the virus is 125 nm. The 3-D structure shows that nucleocapsid protein and nucleic acid are found beneath lipid bilayer [25]. It contains 14 functional open reading frames (ORFs), out of which two ORFs make replicase genes responsible for encoding proteins needed for the synthesis of viral RNA. The other 12 ORFs are responsible for making eight accessory proteins and four structural proteins: membrane, spike, envelope, and nucleocapsid [26, 27]. One of the main virulence factors of coronavirus is N protein, which is highly infectious [28]. The structure of the coronavirus spike is very complex, with three main segments. These three segments consist of a short intracellular tail, single-pass transmembrane anchor, and a large ectodomain. The ectodomain contains a receptor-binding subunit S1 and a membrane-fusion subunit S2. The coronavirus spike on electron microscopy is a clover-shaped trimer with three S1 sections and a trimer. When the coronavirus infects a host cell, it loosely binds to the receptor via the S1 subunit and the S2 subunit connects the ACE-2 receptors on the host cell with the coronavirus cell membrane. This allows for the integration of the coronavirus genome with the host cell genome [19, 29, 30]. ACE2 receptors are present in the nose, lungs, blood vessels, intestines, and certain areas of the brain [31]. It uses Transmembrane protease serine 2 (TMPRSS2) serine protease to prime S protein [32].
Accumulating evidence suggests that SARS-CoV-2 is most likely a zoonotic source from the wet market in Wuhan. A vast number of people were exposed to this animal marketplace. This proposes the idea of the animal to human transmission at some point likely being the primary source of spread [33]. According to Rothan and Byrareddy, SARS-CoV-2 is primarily transmitted via person-to-person direct contact through respiratory droplets by cough and sneezing [33]. Numerous case studies have also indicated the presence of SARS-CoV-2 live viral RNA in feces. This is suggestive that there is a high probability of fecal-oral transmission with SARS-CoV-2 as another possible route of transmission [34]. The novel Coronavirus is a developing situation where through data analysis and time we will be able to understand more possible routes of transmission. According to Qu and colleagues, strong evidence suggests that the coronavirus can thrive for extended lengths of time outside of its host cell. It is also believed that the COVID-19 virus can survive for many hours on a large number of surfaces including sterile sponges, aluminum, or latex materials. This increases the virus’ opportunity for transmission from the external environment into the host cell through contact with the eyes, mouth, and nose [35]. A study by van Doremalen and team analyzed surface integrity and aerosol of SARS-CoV-2 compared to SARS-CoV. This study utilized Bayesian regression to measure the decay rates of both viruses in aerosol and surfaces. COVID-19 showed viability in aerosol for up to 3 hours, with a decay rate of 103.5 to 102.7 Median Tissue Culture Infectious Dose (TCID)50/L . This decay rate was very similar to the decay rate seen in SARS-CoV, which was 104.3 to 103.5 TCID50/mL suggesting that aerosols can remain infectious for several hours and surfaces can remain infectious for up to one day [36].
Every person is at risk to be infected with SARS-CoV-2 if exposed; however, not everyone develops severe, life-threatening infections [37]. Patients who are more susceptible to develop severe infections include patients with comorbidities like diabetes mellitus, chronic obstructive pulmonary disease, interstitial lung disease, chronic heart failure, coronary artery diseases, cardiomyopathies, metabolic syndrome, and hypertension [37]. The older age group (especially above 85 years of age) and with underlying medical conditions like chronic kidney disease, sickle cell disease, cystic fibrosis, cerebrovascular diseases, liver diseases, smoking, thalassemia, neurologic diseases like dementia and immunocompromised state due to transplantation of solid organ, obesity (body mass index 20 or greater), use of steroids/other immunomodulatory drugs, human immunodeficiency virus, blood or bone marrow transplant are also at increased risk [6, 37, 38]. The SARS-CoV-2 life cycle into host cell is shown in Figure 1.
Figure 1. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) spike (S) glycoprotein binds with host cell angiotensin converting enzyme 2 (ACE-2) receptor. Subsequently, the virus enters the host cell either through membrane fusion or endocytosis and releases its positive sense ribonucleic acid (RNA) in the host cell cytoplasm via uncoating. The host ribosomes translate viral polymerase protein from positive sense RNA. The viral polymerase replicates negative sense RNA from the positive sense RNA. The viral polymerase then utilizes negative sense genome to produce more positive sense RNA (genomic replication) and mRNAs for nucleocapsid (N), spike (S), membrane (M), envelope (E) (subgenomic transcription). After the translation of viral structural proteins, S, E, and M proteins are processed in Endoplasmic Reticulum-Golgi (ERG) intermediate compartment. Nucleocapsids are assembled in the cytoplasm and then bud into the lumen of the ERG intermediate compartment. Finally, the mature virus inside the Golgi vesicle is released from the infected cell through exocytosis. A mature virus is capable of infecting the lung, endothelium, intestine, heart, testis, kidney through ACE-2 receptors.
Omega-3 Fatty Acids
Omega-3 FAs might be a safe and relatively inexpensive prophylactic approach for those who are at high risk. For a problem that has arisen from nature, we may return to nature for the cure.
Omega-3 FAs have been investigated repeatedly since 1994 when the tremendous health benefits were first established. They were found to lower the risk of thrombosis in cardiovascular disease and it may impact positively on inflammatory diseases, brain function, and mental health, among a multitude of other benefits [39]. The term omega-3 comes from the structural descriptor for a family of PUFAs. Within the omega-3 FA family, we can find and linolenic acid (LNA) and its derivatives, including α-linolenic acid (ALA), eicosapentaenoic acid (EPA), and docosahexaenoic acid (DHA). All of which are crucial elements for the functions of various cells and organs such as the brain, eyes, cardiovascular system, immune system, and general human growth [40]. In that sense, it has been shown that neural membranes of our neurons contain high concentrations of PUFAs. The omega-3 FAs belong to the essential fatty acid group within the PUFAs family and previous studies have demonstrated that our bodies cannot synthesize them. Therefore, they must be obtained from the diet [41].
Extensive evidence has been published about levels of omega-3 PUFAs that can mediate anti-inflammatory effects [9, 40, 41, 42, 43]. For example, omega-3 FAs play a role in mediating inflammatory processes and immunomodulation for both innate and acquired immune systems [9]. Also, a study done by Chanda and team concluded that omega-3 FAs could be a potential antimicrobial drug with little potential for drug resistance [44]. However, the use of these fatty acids as antimicrobial agents has not yet received much attention in clinical medicine worldwide.
Nowadays, the novel coronavirus has resulted in a pandemic that has spread with sheer rapidity across the globe. In this literature review, we provide information on omega-3 FAs and the possible use of this natural, inexpensive, and safe compound as an alternative treatment for those who are at high risk or have contracted the disease.
The principal source of omega-3 FAs in the human diet comes from eating fresh fish, particularly oily fish, including mackerel, salmon, herring, flounder, cod, and mullet, as shown in Table 2. This happens because most fish foods such as microalgae and other invertebrates are rich in DHA and EPA [45]. Besides this, most microorganisms such as marine protists and dinoflagellates, such as species of Thraustochytrium, Schizochytrium, and Crypthecodinium are rich sources of DHA. On the other hand, microalgae like Phaeodactylum and Monodus are sources rich in EPA [45]. However, we also can find omega-3 amounts in non-marine foods such as cereals, seeds, nuts, and some fruits and vegetables [46, 47].
Omega-3 FAs are PUFAs that are abundantly available in nature. Various forms in which fatty acids exist are free fatty acids (FFAs), ethyl esters, triglycerides, and phospholipids [47, 48]. Dietary lipids after ingestion are hydrolyzed in the intestinal lumen. FFAs and monoglycerides are hydrolysis products that are incorporated into micelles that contain bile salt and get absorbed in enterocytes mostly by passive diffusion [49]. Within the enterocytes, FFAs get incorporated in chylomicrons and via lymphatic circulation will enter the circulation from where lipids are delivered to various organs for further oxidation, storage, or metabolism [49]. Factors like intestinal pH, bile secretion, microorganisms, type of chemical bond, concomitant food intake and presence of some other components like calcium affects the absorption and thus the bioavailability. A diet that consists of FFAs has a higher bioavailability than an ester [50]. Absorption of EPA in triglyceride form is 90% whereas it is 60% in the form of ethyl ester [46]. ALA has low bioavailability due to a higher rate of oxidation, whereas DHA is more bioavailable as a result of being a poor β-oxidation substrate [50]. Binding of long-chain omega-3 FAs in sn-⅓ position to glycerol increases bioavailability by facilitating the bond’s lipase hydrolysis. A study on hamsters conducted by Cholewski and colleagues, showed that DHA when present in sn-2 position facilitates the absorption of fatty acids in the intestine and its tissue incorporation [51]. Metabolism occurs mainly in the liver [52]. ALA gets converted to EPA and DHA by process of desaturation and elongation [53, 54]. Studies show that in healthy young men, approximately 8% of dietary ALA is converted to EPA and 0 – 4% is converted to DHA. Whereas in healthy young females, 21% dietary ALA is converted to EPA and 9% to DHA [55]. ALA with the help of Δ6-desaturase forms Stearidonic acid which then forms Eicosatetraenoic acid via elongation. EPA and DHA are formed by desaturation with the help of Δ5-desaturase [50]. The half-life of EPA is 37 hours and that of DHA is 46 hours [52].
EPA binds and activates PPARα whereas DHA binds and activates PPARγ [56]. When omega-3 FAs are incorporated into the cell membrane, it induces production of eicosanoids and resolvins which then compete with arachidonic acid for the activity of phospholipase A2. FAs are then liberated inside the cytosol and via cyclooxygenase-2 (COX-2), 5-lipoxygenase and thromboxane synthetase activity gets degraded into PGs, LTs, and TX respectively. Thus, omega-3 FA is responsible for decreasing the synthesis of eicosanoids derived from arachidonic acid (AA) like PGI2, PGF2α, PGE2, and LTB4 which are responsible for pro-inflammatory responses and increase the synthesis of LT5 and PGE3 from EPA which have weak effects on inflammation [57, 58].
The guidelines have remained unchanged since 2003 when the American Heart Association recommended consuming at least 0.5 g/day of omega-3 FA to prevent the risk of cardiovascular disease [59]. Despite this, a study conducted by Richter and colleagues showed that more than 90% of American people consumed less than the recommended optimal value for omega-3 FAs in the diet (0.17 g/day) [46]. Aside from maintenance of normal health, omega-3 FAs are also recommended in specific dosages for a variety of inflammatory conditions, as mentioned in Table 3.
Omega-3 FAs belong to a category of supplements known as GRAS (generally recognized as safe). Omega-3 FAs will rarely cause a few mild, non-distressing adverse effects such as unpleasant taste, bad breath, and change in body odor. Some mild gastrointestinal symptoms such as nausea, vomiting, loose stools, and increased stool frequency may be associated with omega-3 FAs. Few patients might report neurologic symptoms such as dizziness and insomnia; however, most symptoms are very mild and self-limiting [50, 57]. Elderly people are at risk of bleeding when they combine long chain PUFA such as fish oil with other anticoagulants such as warfarin and aspirin. The anti-atherosclerotic and anti-lipidemic effects of omega-3 FAs are well known; however, in patients who combine warfarin and fish oil supplements, the risk of bleeding is increased due to inhibition of platelet aggregation. This is the reason which leads to irreversible coagulopathy in elderly patients taking the combination even after suffering blunt head trauma [8, 60].
Omega-3 Fatty Acids and Inflammation
A study conducted by Gutierrez and colleagues showed that omega-3 FA is incorporated throughout the body into the bi-phospholipid layer of the cell membrane of neutrophils and produces different mediators such as prostaglandins, leukotrienes, and maresins. So, if the injury occurs the byproducts of those cell membranes may produce less inflammatory provoking mediators compared to omega-6 FAs, which are more prevalent in the Western diet [58]. Sheppard and colleagues showed that children and adults in the US did not consume sufficient EPA and DHA in their diets. In other terms, Western diets predispose to have a high omega-6/omega-3 ratio which may promote the pathogenesis of many diseases [61, 62]. Further, there is evidence that omega-6 may inhibit the anti-inflammatory effect of omega-3 FAs [63].
Previous studies have been done to clarify the role of omega-3 on anti-inflammatory mechanisms. For example, Saifullah and colleagues carried out a study to know the outcomes of adding EPA and DHA to the diet of hemodialysis patients for 3 months, showing a modest reduction in serum C-reactive protein, which is an inflammatory mediator produced in the liver in response to inflammation [10].
Microorganisms like bacteria, viruses, fungi, protozoa, and worms can all cause infections. Sepsis may occur following infections which can disturb the homeostasis of the body leading to uncontrolled inflammation and ultimately organ failure, shock, and death. A study was done with omega-3 FA lipid emulsion in the cases of sterile peritonitis and murine polymicrobial sepsis demonstrated anti-inflammatory properties of omega-3 FAs. In this study, omega-3 FAs reduced neutrophil infiltration, pro-inflammatory mediators, and classical monocytes while it enhanced non-classical monocyte/macrophage recruitment and efferocytosis in sepsis [64].
Omega-3 FAs include EPA and DHA. Saedisomeolia and colleagues conducted a study to determine the anti-inflammatory properties of DHA and EPA in airway epithelial cells infected with Rhinovirus. In this study, the researchers incubated airway epithelial cells with EPA, DHA, and AA for 24 hours and then infected them with rhinovirus for 48h. They measured IL-6, IL-8, and interferon-gamma-induced protein-10 (IP-10) released by cells using enzyme-linked immunosorbent assay. The investigators found that DHA significantly reduced the release of IL-6 and IP-10 from the cells infected with different strains of rhinovirus. This could be explained by the efficiency of omega-3 FA reducing inflammation by inhibiting AA metabolism to eicosanoids and finally reducing pro-inflammatory cytokines and immune cell function [65].
Omega-3 Fatty Acids and Oxidative Stress
Omega-3 FAs have been found to exhibit antioxidant activity through various mechanisms including upregulating nuclear factor erythroid 2-related factor 2 (NRF2) mediated antioxidant effects, reducing F2 isoprostanes formed during the oxidation of arachidonic acid, inducing PPARγ and modulating toll-like receptor 4 (TLR4) receptors which all lead to a reduction in κβ phosphorylation and thus reduce NF-κβ which in turn reduces inflammatory markers like IL-6, TNFα, and tissue growth factor beta (TGFβ). They also induce mitogen activated protein kinase (MAPK) phosphatases and upregulate glutathione also known as GSH, which is an antioxidant molecule, and upregulate genes responsible for the production of heme-oxygenase, which is cytoprotective. N-3 fatty acids also inhibit lipid peroxidation. They are ultimately metabolized to anti-inflammatory molecules like resolvins, protectins, and maresins [66, 67, 68].
Omega-3 Fatty Acids and Immune System
There is a plethora of ongoing research on the effects of omega-3 FAs and its modifications to the immune system. Omega-3 FAs are considered to be a polyunsaturated fatty acid, which upregulates the activation of immune cells specifically in macrophages, neutrophils, T-cells, B-cells, dendritic cells, natural killer cells, mast cells, basophils, and eosinophils. Omega-3 FA plays a role in the host cellular membrane which regulates membrane fluidity and intricate lipid raft assembling [9]. This is demonstrated in the Figure 2.
Figure 2. How omega-3 fatty acids impact the cellular immune response.Nuclear factor kappa B (NF-κB) is a pro-inflammatory cytokine triggering an inflammatory response via activation of transcription of genes for further pro-inflammatory proteins. Omega-3 fatty acids potentially exert their anti-inflammatory effect via toll-like receptor 4 (TLR4) pathway and G-protein coupled receptor 120 (GPR120) pathway to inhibit the NF-κB and consequently the inflammatory cascade. TAB, TGF-beta activated kinase; TAK, tat-associated kinase; IRAK, interleukin 1 receptor-associated kinase; TRAF6, tumor necrosis factor receptor associated factor 6; TRIAP, TP53 regulated inhibitor of apoptosis; MD2, myeloid differentiation factor 2.
Omega-3 FAs also increase the function of neutrophils which are the first responders of infection in the body. The study showed that omega-3 FAs incorporate phospholipids of the cell membrane of neutrophils and produce different mediators such as prostaglandins, leukotrienes, and maresins. In addition, neutrophils strengthen the immune function by promoting neutrophil migration, phagocytic capacity, and production of reactive free radicals to kill microbes. Omega-3 FAs help activate the function of T cells by promoting antigen-presenting cells (APC), for example, macrophages or dendritic cells. Subsequently, that promotes activation of different subgroups of T cells such as CD4 cells, Th17 cells, and regulatory T cells. B cells are also activated by omega-3 FAs, producing more antibodies utilizing heavy chain immunoglobulin rearrangements and further differentiation. The study claims that omega-3 FAs also increase the population of B cells in the study mice [9]. Omega-3 improves the function of the macrophages by secreting cytokines and chemokines, promoting the ability of phagocytosis, and activating macrophages by polarization [69].
Moreover, the omega-3 FA has appeared to block the activity of NF-κB through decreasing the degradation of the inhibitory subunit of the NF-κB called IkB, in cultured pancreatic cells and human monocyteds. Since NF-κB is responsible for cytokine production in immune cells, by blocking that pathway, its decreasing cytokine storm, and complication [70]. Omega-3 FAs are also known to down-regulate NF-κB. NF-κB is considered to be a transcription factor involved in cell signaling to initiate an inflammatory response by the innate immune system. Furthermore, omega-3 FAs intake upregulates vagal response which in turn down-regulates inflammation and cytokine production. To our understanding omega-3 FAs have multiple effects on the inflammatory response; however, analytic data has not yet recognized its role in critically ill patients. Future research may indicate that supplementation of omega-3 FA fish oils may play a crucial role in SARS-CoV-2 treatment [71].
Omega-3 Fatty Acids and Viral Infection
Omega-3 FAs could be a potential antimicrobial drug with little potential for drug resistance [72]. The metabolites of both omega-3 and omega-6 play an important role in the synthesis of different mediators such as prostaglandins, leukotrienes, thromboxanes, protectins, and resolvins [9]. The study shows that fish oil enhances antiviral response by inducing interferon (IFN) which inhibits viral replication [69]. The anti-inflammatory effect by omega-3 FAs is stronger in DHA compared to that of EPA, and their secretion of cytokines IL-10 is further increased by omega-3. CD8 T cells are responsible for fighting against viruses by inducing the production of different cytokines in the body, such as Tumor Necrosis Factor-alpha (TNF-alpha) and granzyme B. However, the surge of cytokines by CD8 T cells to defend influenza viruses impose unintended lung damage and further deteriorate the clinical outcome. Omega-3 FAs weaken the antiviral response by CD8 T cells and could potentially be used to modulate cytokine responses as antiviral responses, and this process is further explained in Figure 3 [73].
Figure 3. Omega-3 fatty acid acting on different elements of the immune response.Omega-3 fatty acids, through their anti-inflammatory mechanism, inhibit the production of pro-inflammatory mediators like interleukin (IL)-1β, IL-6, tumor necrosis factor (TNF)-α and prevent cytokine storm. Some studies also suggest that they dampen the inflammatory response through regulatory T cells (Treg) differentiation. They also exert an anti-viral effect by enhancing the phagocytic activity of cells of the innate immune system- Neutrophils and Macrophages.
Other Benefits of Omega-3 Fatty Acids
Omega-3 PUFAs include α-linolenic acid (ALA; 18:3 ω-3), stearidonic acid (SDA; 18:4 ω-3), eicosapentaenoic acid (EPA; 20:5 ω-3), docosapentaenoic acid (DPA; 22:5 ω-3), and docosahexaenoic acid (DHA; 22:6 ω-3). The health benefits of omega-3 FA are encompassing and cover a wide range of different organ systems and targets including cardiovascular disease, diabetes, cancer, Alzheimer’s disease, dementia, depression, visual and neurological development, and maternal and child health. Numerous studies have been done that enumerate the reduction in clinical disease rates and mortality rates in patients suffering from a vast array of diseases. Research has been conducted involving humans and omega-3 FA for well over 40 years [74]. Albert and colleagues demonstrated that diets rich in fish and seafood containing high levels of omega-3 PUFAs lead to a statistically significant reduction in mortality from cardiovascular events. The study population included Inuit people who had a diet naturally predominated by seafood and marine life. Men who consumed fish at least once every seven days had a multivariate relative risk of sudden death of 0.48 (95% confidence interval, 0.24 – 0.96; P = 0.04) compared to men who consumed fish less frequently than once per month, demonstrating that diets rich in omega-3’s can reduce the risk of death for men from the cardiovascular event by half [11]. Omega-3 supplementation has also been studied in the setting of ARDS. In a study done in 2015, it was determined that natural antioxidants like omega-3 only lead to a statistically significant decrease in mortality in those suffering from ARDS [75]. Due to the survival rate of COVID-19 patients suffering from ARDS standing at 25%, it is therefore imperative that methods that could potentially provide therapeutic relief or treatment are investigated thoroughly [12]. Although the role of ω-3 supplementation in ARDS needs to be further elucidated, its vital role in reducing reactive oxygen species and pro-inflammatory cytokines, such as TNF-α, IL-1β, IL-6, and IL-8, is widely documented. Therefore, ω-3 PUFAs could be considered for potential interventions for COVID-19 [75].
Omega-3 index, which is the EPA + DHA, is a a percent of total red blood cell fatty acid and is regarded as a new risk factor for death from coronary heart disease (CHD) (Fig. 2). The value of about 8% is estimated to be cardioprotective while that of less than 4% is associated with an increased risk of CHD death [76]. As per our discussion, omega-3 FAs are less prone to the production of different inflammatory markers compared to omega-6 that could initiate a cascade of the cytokine storm. It is evident that the regions with a low index like the USA, few European countries experiencing higher COVID-19 related deaths than those with high index. Omega-3 FAs may play a role in COVID-19 by reducing inflammatory markers and may lower the coronary complications. Figure 4 shows the Global View of Omega-3 Index Levels.
Figure 4. The global view of omega-3 index levels is shown in this figure.The omega-3 index risk zones are as follows: ● High Risk ≤ 4%. ● Intermediate risk = 4 – 8%. ● Low risk > 8%.
Conclusion
There are various benefits of omega-3 FA and taking it as a supplement might be associated with the prevention of the viral entry by changing the composition of fats in the bilipid membrane of cells. Omega-3 FAs, such as DHA and EPA, perform their role by being incorporated in the cell membrane and affecting the clumping of toll-like receptors and thus preventing signals that activate NF-κB and help to ameliorate complications of COVID-19 by producing fewer pro-inflammatory mediators. DHA and EPA are precursors of particles called resolvins D and E, which reduce the proinflammatory mediators thereby reducing pulmonary neutrophils recruitment, increasing apoptosis by macrophages, and subsequently decreasing broncho-alveolar IL-6 production and as a result, decreasing inflammation of the lung. Omega-3 FA plays a role in increasing the phagocytic capacity of macrophages due to the changes in the composition of the cell membrane bilipid layer. Omega-3 FAs also play a role in mediating inflammatory processes and immunomodulation for both innate and acquired immune systems.
It is necessary to understand that the link between omega-3 FA-rich diet and the clinical outcome could be far more complex than previously considered when treating COVID-19 patients. At the very least, this information could serve as the impetus that initiates further conversation and investigation into dietary supplementation that can be considered in both hospitalized patients and patients at home. Several clinical trials are being conducted to investigate the most appropriate treatment for SARS-CoV-2. Due to its anti-inflammatory, immunomodulatory, and other various beneficial properties, omega-3 FA is a natural, inexpensive, and could play a role as a healthier choice of supplement during this ongoing pandemic situation. Future larger randomized blinded clinical trials are warranted and sufficient confirmatory results are required which could further shed light on this topic.
Research shows people with high omega-3 index less likely to die from COVID-19
Pilot study shows positive outcomes for those suffering from COVID-19
Researchers with the Fatty Acid Research Institute (FARI) and collaborators at Cedars-Sinai Medical Center in Los Angeles and in Orange County, CA, have published the first direct evidence that higher omega-3 blood levels may reduce risk for death from COVID-19 infection. The report was published in the journal Prostaglandins, Leukotrienes and Essential Fatty Acids on January 20, 2021.
There are several papers in the medical literature hypothesizing that omega-3 fatty acids should have beneficial effects in patients with COVID-19 infection, but up until now, there have been no published peer-reviewed studies supporting that hypothesis.
This study included 100 patients admitted to the hospital with COVID-19 for whom admission blood samples had been stored. Clinical outcomes for these patients were obtained and blood was analyzed for the Omega-3 Index (O3I, red blood cell membrane EPA+DHA levels) at OmegaQuant Analytics (Sioux Falls, SD). Fourteen of the patients died.
The 100 patients were grouped into four quartiles according to their O3I, with 25% of the patients in each quartile. There was one death in the top quartile (i.e., 1 death out of 25 patients with O3I>5.7%), with 13 deaths in the remaining patients (i.e., 13 deaths out of 75 patients with O3I<5.7%).
In age-and-sex adjusted regression analyses, those in the highest quartile (O3I >5.7%) were 75% less likely to die compared with those in the lower three quartiles (p=0.07). Stated another way, the relative risk for death was about four times higher in those with a lower O3I (<5.7%) compared to those with higher levels.
“While not meeting standard statistical significance thresholds, this pilot study – along with multiple lines of evidence regarding the anti-inflammatory effects of EPA and DHA – strongly suggests that these nutritionally available marine fatty acids may help reduce risk for adverse outcomes in COVID-19 patients. Larger studies are clearly needed to confirm these preliminary findings,” said Arash Asher, MD, the lead author on this study.
Agreeing with Dr. Asher, cardiology researcher and co-developer with Dr. Harris of the Omega-3 Index, Clemens von Schacky, MD, (CEO, Omegametrix GmbH, Martinsried, Germany, and not involved with the study) said, “Asher et al have demonstrated that a low Omega-3 Index might be a powerful predictor for death from COVID-19. Although encouraging, their findings clearly need to be replicated.”
Omega-3 expert James H. O’Keefe, Jr., MD, (Director of Preventive Cardiology, Saint Luke’s Mid America Heart Institute, Kansas City, MO, and also not involved with the study) observed, “An excessive inflammatory response, referred to as a ‘cytokine storm,’ is a fundamental mediator of severe COVID-19 illness. Omega-3 fatty acids (DHA and EPA) have potent anti-inflammatory activities, and this pilot study provides suggestive evidence that these fatty acids may dampen COVID-19’s cytokine storm.”
The FARI research team is currently seeking funding to expand upon these preliminary observations. Individuals and organizations that want to support this research are encouraged to visit FARI’s donations page.
The Fatty Acid Research Institute (FARI) is a non-profit research and education foundation. FARI was founded in order to accelerate discovery of the health effects of fatty acids, most notably, the long chain omega-3 fatty acids EPA and DHA. FARI researchers and scientists will focus single-mindedly on publishing high-quality research studies on the multiple relationships between fatty acid levels and human (and animal) health outcomes. These studies will improve the ability to predict risk for disease, and more importantly, suggest ways to reduce risk by changing our diets and/or supplementation regimens.
ChooseLife Notes:
Again, this builds the picture out, that likelihood of acquiring and gradient of infection are both clearly linked to multiple biological processes, these processes are demonstrably underpinned in many instances, or enhanced greatly in others, by the intelligent adaptation of diet to include plentiful amounts of Omega3, my preference is FlaxOil via Budwig, it adds so many extra facets, partcularly in Mucin production and intestinal fauna well-being (but I am perhaps biased a little as a vegetarian!).
The chronic and low-grade inflammation induced by obesity seem to be the “first hit” to retinopathy associated to diabetes type 2. Herein, we hypothesized that omega-3 fatty acids from flaxseed oil enriched diet disrupt the pro-inflammatory status in the retina, protecting against retinopathy development. For eight weeks under a high-fat diet (HF), several physiological parameters were monitored to follow the metabolic homeostasis disruption. After this period, mice were treated with a HF substituted in part of lard by flaxseed oil (FS) for another eight weeks. Food behavior, weight gain, glucose and insulin sensitivity, electroretinography, RT-qPCR and western blots were carried out. The HF was able to induce a pro-inflammatory background in the retina, changing IL1β and TNFα. VEGF, a master piece of retinopathy, had early onset increased also induced by HF. The FS-diet was able to decrease inflammation and retinopathy and improved retinal electro stimuli compared to HF group. GPR120 and GPR40 (G Protein-Coupled Receptors 120 and 40), an omega-3 fatty acid receptors, were detected in the retina for the first time. FS-diet modulated the gene expression and protein content of these receptors. Thus, unsaturated fatty acids protect the retina from diabetes type 2 mice model from disease progression.
The current coronavirus disease 2019 (COVID-19) pandemic presents a global challenge for managing acutely ill patients and complications from viral infection. Systemic inflammation accompanied by a “cytokine storm,” hemostasis alterations and severe vasculitis have all been reported to occur with COVID-19, and emerging evidence suggests that dysregulation of lipid transport may contribute to some of these complications. Here, we aim to summarize the current understanding of the potential mechanisms related to COVID-19 dyslipidemia and propose possible adjunctive type therapeutic approaches that modulate lipids and lipoproteins. Specifically, we hypothesize that changes in the quantity and composition of high-density lipoprotein (HDL) that occurs with COVID-19 can significantly decrease the anti-inflammatory and anti-oxidative functions of HDL and could contribute to pulmonary inflammation. Furthermore, we propose that lipoproteins with oxidized phospholipids and fatty acids could lead to virus-associated organ damage via overactivation of innate immune scavenger receptors. Restoring lipoprotein function with ApoA-I raising agents or blocking relevant scavenger receptors with neutralizing antibodies could, therefore, be of value in the treatment of COVID-19. Finally, we discuss the role of omega-3 fatty acids transported by lipoproteins in generating specialized proresolving mediators and how together with anti-inflammatory drugs, they could decrease inflammation and thrombotic complications associated with COVID-19.
Within the secreted phospholipase A2 (sPLA2) family, group X sPLA2 (sPLA2-X) has the highest capacity to hydrolyze cellular membranes and has long been thought to promote inflammation by releasing arachidonic acid, a precursor of pro-inflammatory eicosanoids. Unexpectedly, we found that transgenic mice globally overexpressing human sPLA2-X (PLA2G10-Tg) displayed striking immunosuppressive and lean phenotypes with lymphopenia and increased M2-like macrophages, accompanied by marked elevation of free ω3 polyunsaturated fatty acids (PUFAs) and their metabolites. Studies using Pla2g10-deficient mice revealed that endogenous sPLA2-X, which is highly expressed in the colon epithelium and spermatozoa, mobilized ω3 PUFAs or their metabolites to protect against dextran sulfate-induced colitis and to promote fertilization, respectively. In colitis, sPLA2-X deficiency increased colorectal expression of Th17 cytokines, and ω3 PUFAs attenuated their production by lamina propria cells partly through the fatty acid receptor GPR120. In comparison, cytosolic phospholipase A2 (cPLA2α) protects from colitis by mobilizing ω6 arachidonic acid metabolites, including prostaglandin E2. Thus, our results underscore a previously unrecognized role of sPLA2-X as an ω3 PUFA mobilizer in vivo, segregated mobilization of ω3 and ω6 PUFA metabolites by sPLA2-X and cPLA2α, respectively, in protection against colitis, and the novel role of a particular sPLA2-X-driven PUFA in fertilization.
ChooseLife : Yet more evidence, of the beneficial properties imbued in individuals, who choose to pay head to Budwig et al. and seek to gain a better balance in their Omega3 to Omega6 ratios. I wouldn’t be without my Flaxoil/Flaxseeds, neither would my… too much!
Americans are undeniably great consumers of added sugar. The average person’s intake is over 126 grams of sugar daily which is way too much. Sugar per se is not harmful but too much of it is detrimental to health. High sugar consumption has long been linked to weight gain, and the development of obesity and lifestyle diseases such as heart disease and diabetes. More recent studies show that sugar can also induce memory problems and neuroinflammation.
A study conducted at the University of Southern California (USC) revealed that intakse of high fructose corn syrup (HFCS) at levels similar to those in commonly available sugary beverages can trigger memory problems and brain inflammation. In the study, adolescent rats consuming high quantities of HFCS were subsequently found to have impaired hippocampal-dependent spatial learning and memory when subjected to the Barne’s Maze test. Rats consuming a sucrose solution experienced moderate learning impairment. Adult rats given either HFCS or sucrose did not show any problems with spatial learning, glucose tolerance or neuroinflammatory markers. According to Scott Kanoski, one of the proponents of the research, the brain is vulnerable to dietary influences during critical periods of development, like adolescence. He further explained that a diet high in added sugar can not only cause weight gain and metabolic problems, but also impair brain function and cognitive ability.
This is supported by an earlier study at the University of California in Los Angeles (UCLA) that tested the effects of fructose and omega-3 fatty acid consumption among rats. Two groups of rats were initially trained to find their way out of a maze. The results showed that long-term consumption of a high fructose diet by the rats negatively affected their cognitive function and ability to recall while omega 3 fatty acids were able to counteract those effects. After six weeks, the rats that consumed fructose forgot the previously learned escape route and developed signs of insulin resistance. The impaired learning and memory problems exhibited by this group of rats was attributed to insulin’s inability to regulate how cells use and store sugar.
Sucrose and high fructose corn syrup are liquid sweeteners often added to processed foods and common beverages such as soft drinks and juices. These added sugars are quickly absorbed in the blood where it lowers the production of brain-derived neurotrophic factor (BDNF), a substance known to influence the formation of new memories and regulate learning. Individuals with impaired glucose tolerance were found to have low levels of this chemical. Low levels of BDNF have also been associated with depression and dementia.
So before you drink your favorite juice or munch on a delectable dessert, remember that added sugars from such beverage and food items are likely culprits for health complications including poor memory and cognitive damage. Avoiding foods with added sugars will help you stay fit and keep your mind healthy.