Authors: Grace Russell,1*Alexander Nenov,2 John T. Hancock1 1. Department of Applied Sciences, University of the West of England, Bristol, UK 2. Water Fuel Engineering, Liquorice Way, Pontefract, UK *Correspondence to Grace2.Russell@live.uwe.ac.uk Disclosure: Dr Nenov is a board member of Water Fuel Engineering. The remaining authors have declared no conflicts of interest. Received: 03.02.21 Accepted: 16.03.21
Abstract
Oxy-hydrogen gas (HHO) is a gaseous mixture of molecular hydrogen and molecular oxygen that is generated by the electrolysis of water and delivered in a 2:1 ratio (66% and 33%, respectively) through the use of noninvasive inhalation devices such as nasal cannulas or nebulisers. Although there is a paucity of scientific evidence supporting this new and emerging therapy, initial investigations indicate that HHO proffers cytoprotective qualities, typically by reducing oxidative stress and attenuating the inflammatory response. These aspects are particularly favourable when considering respiratory medicine because underlying inflammation is known to drive the pathological progress of numerous respiratory conditions, including asthma, chronic obstructive pulmonary disorder, and, pertinently, coronavirus disease (COVID-19). Direct delivery to the lung parenchyma is also likely to increase the effectiveness of this emerging medical therapy.
This narrative review aims to delineate how this particular combination of gases can affect cellular processes at the molecular level by focussing on the evolutionary requirement for both oxygen and hydrogen. Furthermore, the authors assess the current available data for the safety and efficacy of HHO in a clinical setting.
ChooseLife : We have a nebuliser and use it now and again, with 1% or so H2O2, but personally think small sips of Milk of Magnesia (pH 11.5) to coat the throat, bring the pH up and let the body start healing itself is best (the Magnesium is shown to loosen sticky mucous), though I am positive towards this research.
Wenju Lu, Xiaoqing Liu, Tao Wang, Fei Liu, Airu Zhu, and Yongping Lin
Patients with coronavirus disease 2019 (COVID-19) exhibit a spectrum of respiratory symptoms like cough and dyspnea.1–3 Airway mucus is an adhesive viscoelastic gel composed mostly of high-molecular-weight mucous glycoproteins and water, which is important in maintaining lung function and health, pathological mucus hypersecretion may cause airway obstruction and lead to respiratory distress. Mucin (MUC) glycoproteins are the major macromolecular components of mucus, which are classified into two major types: the gel-forming secreted MUC5AC and the membrane-tethered MUC1.4 Here, with an attempt to understand the lung changes, we sought to provide a delineation of the components of airway mucus from patients with COVID-19.
To clean airway obstruction, respiratory tract mucus was aspirated and collected via bronchoscopy from COVID-19 patients with a critical illness, and optical coherence tomography (OCT) was applied via bronchoscopy to obtain cross-sectional images of the bronchiole. For healthy control, sputum was induced by inhaled hypertonic (3%) saline solution delivered with an ultrasonic nebulizer. After collection, sputum was processed as previously described for components analysis.5 Medical history, and clinical and laboratory data of the participants were extracted from electronic medical records. The study was approved by the Ethics Committee of the First Affiliated Hospital of Guangzhou Medical University (No. 2020-65). The requirement for informed consent was waived because the study was observational and the family members were in quarantine.
MUC5AC (sc-21701; Santa Cruz, Shanghai, China) and MUC1 (sc-6827; Santa Cruz) in airway mucus were measured using enzyme-linked immunosorbent assay, and MUC1-cytoplasmic tail (CT, clone EP1024Y; Abcam, Shanghai) levels were measured by Western blot analysis as described previously.5 The levels of MUC5AC and MUC1 were normalized to their average signal reading of a healthy control group.
A total of 16 patients with COVID-19 were included in this study, the clinical characteristics of the recruited subjects were shown in Table S1. There was no significant deviation in the distribution of age, or sex between the cohorts of case and control subjects. All the patients with COVID-19 were admitted to the intensive care unit because of low oxygenation index (199 ± 23 mm Hg), and 79% of them received mechanical ventilation. Blood laboratory tests showed elevated inflammatory indexes including leukocyte count, C-reactive protein, and interleukin-6 in most of the patients with COVID-19 (Table S2).
OCT indicated clear bronchiole in healthy controls (Figure 1A) and mucus retention in the bronchiole of patients with COVID-19 (Figure 1B). A volume of 1-8 mL white to gray sputum with high viscosity (Figure 1C) was aspirated from the respiratory tract of 16 patients with COVID-19. Induced sputum from healthy control was clear and transparent with low viscosity. Compared to healthy control, airway mucus from patients with COVID-19 had a higher level of MUC5AC (Figure 1D), MUC1 (Figure 1E), and MUC1-CT fragment (Figure 1F). However, there were no significant differences in the concentration of total protein, sodium, or chloride in the airway mucus from patients with COVID-19 when compared to healthy control (Table S3).
Representative cross-sectional images of bronchioles in (A) healthy and (B) critical ill COVID-19 patients were obtained with optical coherence tomography and bronchoscopy. C, Airway mucus aspirated by bronchoscopy. D, MUC1 and (E) MUC5AC protein levels as measured by ELISA, and (F) MUC1-CT level as measured by Western blot analysis in the airway mucus from COVID-19 patients and healthy control (HC). The levels of MUC5AC and MUC1 were normalized to their average signal reading of healthy control group. COVID-19, coronavirus disease 2019; CT, cytoplasmic tail; ELISA, enzyme-linked immunosorbent assay; MUC, mucin
Although more than half of patients with COVID-19 presented with a dry cough,6 this study provided direct evidence showing mucus retention in the small airway of patients with COVID-19, and patients were not able to expectorate by themselves and need bronchoscopy aspiration to help them to clean respiratory tract. The sputum from these patients with COVID-19 was viscous, which is not surprising as MUC5AC levels are extremely high, hyperconcentration of this gel-forming MUC dehydrates airway surfaces and causes mucus adhesion, which may contribute to airflow obstruction and respiratory distress. Clearance of airway mucus is an important way to increase oxygen and carbon dioxide exchange, bronchoscopy aspiration of airway mucus was used in all our patients to relieve hypoxia. In our center, all the 16 critical ill COVID-19 patients recovered and were discharged from hospitalization, which may attribute to our aggressive clearance of the respiratory tract. It is of note that bedside bronchoscopy may not be available in some hospitals as the medical resources are limited during the COVID-19 pandemic, carbocisteine has been reported to inhibit airway MUC5AC secretion, which could be used to reduce sputum viscosity and elasticity in patients with COVID-19. In addition, hydration of sputum by aerosolized hypertonic saline solutions or mannitol, and dilation of bronchi via aerosolized salbutamol may facilitate sputum expectoration.
MUC1 is a membrane-tethered MUC expressed on the apical surface of epithelial cells.7, 8 Since MUC1-CT fragment is on the cytoplasmic side of the cells, the elevated sputum CT fragment in patients with COVID-19 could come from detached and disrupted epithelial cells, which is evidenced by the pathological findings of diffuse alveolar damage with fibromyxoid exudates and macrophage infiltration in the lung tissue from patients with COVID-19.9
The limitation of this study is that induced sputum was used in the control group to compare airway mucus aspirated via bronchoscopy from patients with COVID-19, because it was very difficult for the patients with COVID-19 to expectorate sputum even with hypertonic saline solution inhalation.
The findings may suggest that increased level of MUCs in the airway mucus may contribute to the high viscosity of airway mucus and sputum retention in the small airway of patients with COVID-19, airway mucus clearance may be indicated to relieve respiratory distress, and MUC5AC may serve as a target for mucolytic agents in treating COVID-19. And MUC1-CT may serve as an indicator reflecting the severity of airway and alveolar epithelial cell damage.
ACKNOWLEDGMENTS
This study was supported by grants from the National Key R&D Project (2016YFC0903700 and 2016YFC1304102), the National Natural Science Foundation of China (81520108001 and 81770043), and grant specific for COVID-19 study from Guangzhou Institute of Respiratory Health. The authors would like to thank Dr Kwang Chul Kim (University of Arizona) for the invaluable assistance with the manuscript.
CONFLICT OF INTERESTS
The authors declare that there are no conflict of interests.
Donald Hathaway III, Krunal Pandav, Madhusudan Patel, Adrian Riva-Moscoso, Bishnu Mohan Singh, Aayushi Patel, Zar Chi Min, Sarabjot Singh-Makkar, Muhammad Khawar Sana, Rafael Sanchez-Dopazo, Rockeven Desir, Michael Maher Mourad Fahem, Susan Manella, Ivan Rodriguez, Alina Alvarez and Rafael Abreu
Corresponding Author: Donald Hathaway III, BSc. Division of Research & Academic Affairs, Larkin Health System, 7031 SW 62nd Avenue, South Miami, FL 33143, USA. Email: donald.hathawayiii@gmail.com
Infect Chemother. 2020 Dec
Abstract
The rapid international spread of severe acute respiratory syndrome coronavirus 2 responsible for coronavirus disease 2019 (COVID-19) has posed a global health emergency in 2020. It has affected over 52 million people and led to over 1.29 million deaths worldwide, as of November 13th, 2020. Patients diagnosed with COVID-19 present with symptoms ranging from none to severe and include fever, shortness of breath, dry cough, anosmia, and gastrointestinal abnormalities. Severe complications are largely due to overdrive of the host immune system leading to “cytokine storm”. This results in disseminated intravascular coagulation, acute respiratory distress syndrome, multiple organ dysfunction syndrome, and death. Due to its highly infectious nature and concerning mortality rate, every effort has been focused on prevention and creating new medications or repurposing old treatment options to ameliorate the suffering of COVID-19 patients including the immune dysregulation. Omega-3 fatty acids are known to be incorporated throughout the body into the bi-phospholipid layer of the cell membrane leading to the production of less pro-inflammatory mediators compared to other fatty acids that are more prevalent in the Western diet. In this article, the benefits of omega-3 fatty acids, especially eicosapentaenoic acid and docosahexaenoic acid, including their anti-inflammatory, immunomodulating, and possible antiviral effects have been discussed.
Introduction
The coronavirus disease 2019 (COVID-19), now known the world over, is an emerging respiratory disease that was first identified in December 2019, in Wuhan, the capital of China’s Hubei province. It has since spread globally, resulting in the ongoing COVID-19 pandemic [1, 2]. In December 2019, this world-changing phenomenon began with an outbreak of pneumonia due to an unknown cause in Wuhan, with an epidemiological link to the Huanan Seafood Wholesale Market Place. The World Health Organization (WHO) was notified on December 31, 2019, by the Chinese Health Authorities [1]. The Chinese Center for Disease Control and Prevention identified a novel coronavirus on January 7, 2020, from the throat swab of a patient, which the WHO subsequently named 2019-nCoV [3]. This respiratory disease rapidly spread beyond the borders of China and by February 15, 2020, 26 countries were affected by this disease [4]. Considering this, the WHO declared it a public health emergency of international concern on January 30, 2020 and called for collaborative efforts of all countries to prevent the rapid spread of the virus [5]. Despite these efforts, the virus continued to spread, and the WHO declared it a pandemic on March 11, 2020 [2]. From its first outbreak in Wuhan, through November 13th, 2020, a total of over 52 million laboratory-confirmed cases of COVID-19 along with over 1.29 million associated deaths, have been reported globally [6]. In the United States (US), the total confirmed cases of COVID-19 have surpassed 10 million with over 240,000 deaths as of November 13th, 2020 [6].
The novel COVID-19 infection in humans may cause a wide range of symptoms, while some patients may remain asymptomatic even if they test positive for the virus. Possible clinical presentations may include fever, fatigue, sore throat, dry cough, shortness of breath, body aches, nasal congestion, anosmia, abdominal pain, and diarrhea, but other less common presentations have been reported as well. The minority of patients may however develop severe symptoms and serious complications such as interstitial pneumonia, septic shock, adult respiratory distress syndrome (ARDS), stroke, disseminated intravascular coagulation (DIC), and multi-organ failure (MODS). Strikingly, even asymptomatic patients are believed to be able to spread the disease [7].
Omega-3 fatty acids (FAs) are polyunsaturated fatty acids (PUFAs) that are abundantly available in nature. Omega-3 FAs belong to a category of supplements known as GRAS (generally recognized as safe). The Omega-3 Index Test serves as a measure of the amount of Eicosapentaenoic Acid (EPA) and Docosahexaenoic Acid (DHA) in the blood, especially in the red blood cell membranes. This index shows the ratio of omega-3 FAs to all other fatty acids. A recent study showed that more than 90% of American people consumed less than the recommended optimal value for omega-3 FAs in the diet (0.17 g/day) [8]. The metabolites of both omega-3 and omega-6 play an important role in the synthesis of different inflammatory mediators such as prostaglandins (PG), leukotrienes (LT), thromboxanes (TX), protectins, and resolvins. Omega-3 FA (fatty acid) plays a role in the host cellular membrane which regulates membrane fluidity and intricate lipid raft assembling in the cell membrane. A study conducted by Gutierrez and colleagues showed that omega-3 FA is incorporated throughout the body into the bi-phospholipid layer of the cell membrane of neutrophils and produces different mediators such as prostaglandins, leukotrienes, and maresins [9]. For that reason, if the injury occurs the byproducts of those cell membranes may produce less inflammatory provoking mediators compared to omega-6, which is more prevalent in the American diet [10]. Omega-3 FAs improve the function of the macrophages by secreting cytokines and chemokines, promoting the ability of phagocytosis, and activating macrophages by polarization [11]. Omega-3 FAs are also known to down-regulate Nuclear Factor-κ Beta (NF-κB). NF-κB is considered to be a transcription factor involved in cell signaling to initiate an inflammatory response by the innate immune system. The study shows that fish oil enhances antiviral response by inducing interferon (IFN) which inhibits viral replication [11]. Omega-3 FAs weaken the antiviral response of CD8 T cells and thereby could potentially be used to modulate cytokine responses to viral invaders [12].
A lack of omega-3 FAs in the diet can change the composition of the cell membrane. Every cell needs a healthy, functioning lipid bilayer to facilitate physiological responses and to maintain fluidity. However, the American diet contains high levels of omega-6 FAs as opposed to omega-3. One of the major causes of death in patients infected with severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) is multiorgan failure, which is a result of immune system overdrive causing cytokine storms. The omega-3 FA is known to produce less pro-inflammatory cytokines, therefore increasing omega-3 FA intake in the diet or supplementation could decrease viral entry, promote better immune function, and decrease severity among those who have been diagnosed with COVID-19. As we are still searching for definitive treatment, omega-3 FAs might be a safe and relatively inexpensive prophylactic and treatment approach for those who are at high risk and those who have the disease. This review aims at describing the health benefits of consuming a diet rich in omega-3 FAs in addition to the possible role in COVID-19.
Coronavirus in Humans
Coronaviruses are a family of spherical viruses, and their surfaces are covered with ‘crown-like’ spikes. These viruses are enveloped with single-stranded linear positive-sense RNA genomes. They are classified under the order Nidovirales, family Coronaviridae, and subfamily Orthocoronavirinae [13]. They have the largest genome for RNA viruses and based on genetic and antigenic criteria, they have been divided into four genera: alpha, beta, gamma, and delta Coronaviruses [14]. They have been widely distributed in nature and can affect other species like birds, bats, cats, rodents, pigs, and other mammals [15]. The seven coronaviruses that infect humans are SARS-CoV-2, alphacoronavirus 229E and NL63, and betacoronavirus HKU1, OC43, coronavirus associated with the SARS-CoV and coronavirus associated with respiratory syndrome in the Middle East (MERS -CoV) [16].
A wide range of similarities exists between SARS-CoV and SARS-CoV-2, as shown in Table 1. Both of them belong to the family Coronaviridae [17]. Studies show that there is a 76.47% similarity in amino acid sequences in both of them [18]. Comparison of RNA sequence and protein modeling showed that the domain on the spike protein which is responsible for attaching SARS-CoV-2 to the receptors on the host cell is similar to SARS-CoV [19]. Both use angiotensin-converting enzyme 2 (ACE-2) receptors for entry in the human respiratory epithelium cells [5, 17]. They are transmitted by respiratory droplets and contact with infected people [20, 21] and responsible for causing symptoms like fever, cough, shortness of breath, and fatigue [22]. They cause the appearance of ground-glass opacities on the Chest X-ray. The simple way to prevent them is by hand hygiene, social distancing, and respiratory hygiene [21]. MERS-CoV uses Dipeptidyl peptidase-4 (DPP4), CD26 receptors to attach to the respiratory epithelial cells, and pneumocytes [17].
SARS-CoV, severe acute respiratory syndrome coronavirus; MERS-CoV, Middle East respiratory syndrome coronavirus; SARS-CoV-2, severe acute respiratory syndrome coronavirus-2; N/A, not applicable; ACE-2, angiotensin-converting enzyme 2; DPP4, dipeptidyl peptidase 4; CD26, cluster of differentiation 26.
The basic reproduction number (R0) of COVID-19 is between 1.4 to 2.5 according to the statement based on January 23rd, 2020. R0 is much higher for COVID-19 compared to that of SARS (1.7 – 1.0) and that of MERS (<1). COVID-19 has been a clinical mystery, as of now, with unique epidemiology, pathogenesis, and clinical outcomes [23]. This type of attachment enhances viral fusion to the human cells and atypical severe clinical outcomes in the host. ACE-2 receptors are present in the heart, lungs, gastrointestinal tract, and blood vessels. ACE-2 receptors are the receptors that mediate the viral entry of SARS-CoV-2, causing vasoconstriction, inflammation, and thrombosis [17, 24].
The diameter of the virus is 125 nm. The 3-D structure shows that nucleocapsid protein and nucleic acid are found beneath lipid bilayer [25]. It contains 14 functional open reading frames (ORFs), out of which two ORFs make replicase genes responsible for encoding proteins needed for the synthesis of viral RNA. The other 12 ORFs are responsible for making eight accessory proteins and four structural proteins: membrane, spike, envelope, and nucleocapsid [26, 27]. One of the main virulence factors of coronavirus is N protein, which is highly infectious [28]. The structure of the coronavirus spike is very complex, with three main segments. These three segments consist of a short intracellular tail, single-pass transmembrane anchor, and a large ectodomain. The ectodomain contains a receptor-binding subunit S1 and a membrane-fusion subunit S2. The coronavirus spike on electron microscopy is a clover-shaped trimer with three S1 sections and a trimer. When the coronavirus infects a host cell, it loosely binds to the receptor via the S1 subunit and the S2 subunit connects the ACE-2 receptors on the host cell with the coronavirus cell membrane. This allows for the integration of the coronavirus genome with the host cell genome [19, 29, 30]. ACE2 receptors are present in the nose, lungs, blood vessels, intestines, and certain areas of the brain [31]. It uses Transmembrane protease serine 2 (TMPRSS2) serine protease to prime S protein [32].
Accumulating evidence suggests that SARS-CoV-2 is most likely a zoonotic source from the wet market in Wuhan. A vast number of people were exposed to this animal marketplace. This proposes the idea of the animal to human transmission at some point likely being the primary source of spread [33]. According to Rothan and Byrareddy, SARS-CoV-2 is primarily transmitted via person-to-person direct contact through respiratory droplets by cough and sneezing [33]. Numerous case studies have also indicated the presence of SARS-CoV-2 live viral RNA in feces. This is suggestive that there is a high probability of fecal-oral transmission with SARS-CoV-2 as another possible route of transmission [34]. The novel Coronavirus is a developing situation where through data analysis and time we will be able to understand more possible routes of transmission. According to Qu and colleagues, strong evidence suggests that the coronavirus can thrive for extended lengths of time outside of its host cell. It is also believed that the COVID-19 virus can survive for many hours on a large number of surfaces including sterile sponges, aluminum, or latex materials. This increases the virus’ opportunity for transmission from the external environment into the host cell through contact with the eyes, mouth, and nose [35]. A study by van Doremalen and team analyzed surface integrity and aerosol of SARS-CoV-2 compared to SARS-CoV. This study utilized Bayesian regression to measure the decay rates of both viruses in aerosol and surfaces. COVID-19 showed viability in aerosol for up to 3 hours, with a decay rate of 103.5 to 102.7 Median Tissue Culture Infectious Dose (TCID)50/L . This decay rate was very similar to the decay rate seen in SARS-CoV, which was 104.3 to 103.5 TCID50/mL suggesting that aerosols can remain infectious for several hours and surfaces can remain infectious for up to one day [36].
Every person is at risk to be infected with SARS-CoV-2 if exposed; however, not everyone develops severe, life-threatening infections [37]. Patients who are more susceptible to develop severe infections include patients with comorbidities like diabetes mellitus, chronic obstructive pulmonary disease, interstitial lung disease, chronic heart failure, coronary artery diseases, cardiomyopathies, metabolic syndrome, and hypertension [37]. The older age group (especially above 85 years of age) and with underlying medical conditions like chronic kidney disease, sickle cell disease, cystic fibrosis, cerebrovascular diseases, liver diseases, smoking, thalassemia, neurologic diseases like dementia and immunocompromised state due to transplantation of solid organ, obesity (body mass index 20 or greater), use of steroids/other immunomodulatory drugs, human immunodeficiency virus, blood or bone marrow transplant are also at increased risk [6, 37, 38]. The SARS-CoV-2 life cycle into host cell is shown in Figure 1.
Figure 1. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) spike (S) glycoprotein binds with host cell angiotensin converting enzyme 2 (ACE-2) receptor. Subsequently, the virus enters the host cell either through membrane fusion or endocytosis and releases its positive sense ribonucleic acid (RNA) in the host cell cytoplasm via uncoating. The host ribosomes translate viral polymerase protein from positive sense RNA. The viral polymerase replicates negative sense RNA from the positive sense RNA. The viral polymerase then utilizes negative sense genome to produce more positive sense RNA (genomic replication) and mRNAs for nucleocapsid (N), spike (S), membrane (M), envelope (E) (subgenomic transcription). After the translation of viral structural proteins, S, E, and M proteins are processed in Endoplasmic Reticulum-Golgi (ERG) intermediate compartment. Nucleocapsids are assembled in the cytoplasm and then bud into the lumen of the ERG intermediate compartment. Finally, the mature virus inside the Golgi vesicle is released from the infected cell through exocytosis. A mature virus is capable of infecting the lung, endothelium, intestine, heart, testis, kidney through ACE-2 receptors.
Omega-3 Fatty Acids
Omega-3 FAs might be a safe and relatively inexpensive prophylactic approach for those who are at high risk. For a problem that has arisen from nature, we may return to nature for the cure.
Omega-3 FAs have been investigated repeatedly since 1994 when the tremendous health benefits were first established. They were found to lower the risk of thrombosis in cardiovascular disease and it may impact positively on inflammatory diseases, brain function, and mental health, among a multitude of other benefits [39]. The term omega-3 comes from the structural descriptor for a family of PUFAs. Within the omega-3 FA family, we can find and linolenic acid (LNA) and its derivatives, including α-linolenic acid (ALA), eicosapentaenoic acid (EPA), and docosahexaenoic acid (DHA). All of which are crucial elements for the functions of various cells and organs such as the brain, eyes, cardiovascular system, immune system, and general human growth [40]. In that sense, it has been shown that neural membranes of our neurons contain high concentrations of PUFAs. The omega-3 FAs belong to the essential fatty acid group within the PUFAs family and previous studies have demonstrated that our bodies cannot synthesize them. Therefore, they must be obtained from the diet [41].
Extensive evidence has been published about levels of omega-3 PUFAs that can mediate anti-inflammatory effects [9, 40, 41, 42, 43]. For example, omega-3 FAs play a role in mediating inflammatory processes and immunomodulation for both innate and acquired immune systems [9]. Also, a study done by Chanda and team concluded that omega-3 FAs could be a potential antimicrobial drug with little potential for drug resistance [44]. However, the use of these fatty acids as antimicrobial agents has not yet received much attention in clinical medicine worldwide.
Nowadays, the novel coronavirus has resulted in a pandemic that has spread with sheer rapidity across the globe. In this literature review, we provide information on omega-3 FAs and the possible use of this natural, inexpensive, and safe compound as an alternative treatment for those who are at high risk or have contracted the disease.
The principal source of omega-3 FAs in the human diet comes from eating fresh fish, particularly oily fish, including mackerel, salmon, herring, flounder, cod, and mullet, as shown in Table 2. This happens because most fish foods such as microalgae and other invertebrates are rich in DHA and EPA [45]. Besides this, most microorganisms such as marine protists and dinoflagellates, such as species of Thraustochytrium, Schizochytrium, and Crypthecodinium are rich sources of DHA. On the other hand, microalgae like Phaeodactylum and Monodus are sources rich in EPA [45]. However, we also can find omega-3 amounts in non-marine foods such as cereals, seeds, nuts, and some fruits and vegetables [46, 47].
Omega-3 FAs are PUFAs that are abundantly available in nature. Various forms in which fatty acids exist are free fatty acids (FFAs), ethyl esters, triglycerides, and phospholipids [47, 48]. Dietary lipids after ingestion are hydrolyzed in the intestinal lumen. FFAs and monoglycerides are hydrolysis products that are incorporated into micelles that contain bile salt and get absorbed in enterocytes mostly by passive diffusion [49]. Within the enterocytes, FFAs get incorporated in chylomicrons and via lymphatic circulation will enter the circulation from where lipids are delivered to various organs for further oxidation, storage, or metabolism [49]. Factors like intestinal pH, bile secretion, microorganisms, type of chemical bond, concomitant food intake and presence of some other components like calcium affects the absorption and thus the bioavailability. A diet that consists of FFAs has a higher bioavailability than an ester [50]. Absorption of EPA in triglyceride form is 90% whereas it is 60% in the form of ethyl ester [46]. ALA has low bioavailability due to a higher rate of oxidation, whereas DHA is more bioavailable as a result of being a poor β-oxidation substrate [50]. Binding of long-chain omega-3 FAs in sn-⅓ position to glycerol increases bioavailability by facilitating the bond’s lipase hydrolysis. A study on hamsters conducted by Cholewski and colleagues, showed that DHA when present in sn-2 position facilitates the absorption of fatty acids in the intestine and its tissue incorporation [51]. Metabolism occurs mainly in the liver [52]. ALA gets converted to EPA and DHA by process of desaturation and elongation [53, 54]. Studies show that in healthy young men, approximately 8% of dietary ALA is converted to EPA and 0 – 4% is converted to DHA. Whereas in healthy young females, 21% dietary ALA is converted to EPA and 9% to DHA [55]. ALA with the help of Δ6-desaturase forms Stearidonic acid which then forms Eicosatetraenoic acid via elongation. EPA and DHA are formed by desaturation with the help of Δ5-desaturase [50]. The half-life of EPA is 37 hours and that of DHA is 46 hours [52].
EPA binds and activates PPARα whereas DHA binds and activates PPARγ [56]. When omega-3 FAs are incorporated into the cell membrane, it induces production of eicosanoids and resolvins which then compete with arachidonic acid for the activity of phospholipase A2. FAs are then liberated inside the cytosol and via cyclooxygenase-2 (COX-2), 5-lipoxygenase and thromboxane synthetase activity gets degraded into PGs, LTs, and TX respectively. Thus, omega-3 FA is responsible for decreasing the synthesis of eicosanoids derived from arachidonic acid (AA) like PGI2, PGF2α, PGE2, and LTB4 which are responsible for pro-inflammatory responses and increase the synthesis of LT5 and PGE3 from EPA which have weak effects on inflammation [57, 58].
The guidelines have remained unchanged since 2003 when the American Heart Association recommended consuming at least 0.5 g/day of omega-3 FA to prevent the risk of cardiovascular disease [59]. Despite this, a study conducted by Richter and colleagues showed that more than 90% of American people consumed less than the recommended optimal value for omega-3 FAs in the diet (0.17 g/day) [46]. Aside from maintenance of normal health, omega-3 FAs are also recommended in specific dosages for a variety of inflammatory conditions, as mentioned in Table 3.
Omega-3 FAs belong to a category of supplements known as GRAS (generally recognized as safe). Omega-3 FAs will rarely cause a few mild, non-distressing adverse effects such as unpleasant taste, bad breath, and change in body odor. Some mild gastrointestinal symptoms such as nausea, vomiting, loose stools, and increased stool frequency may be associated with omega-3 FAs. Few patients might report neurologic symptoms such as dizziness and insomnia; however, most symptoms are very mild and self-limiting [50, 57]. Elderly people are at risk of bleeding when they combine long chain PUFA such as fish oil with other anticoagulants such as warfarin and aspirin. The anti-atherosclerotic and anti-lipidemic effects of omega-3 FAs are well known; however, in patients who combine warfarin and fish oil supplements, the risk of bleeding is increased due to inhibition of platelet aggregation. This is the reason which leads to irreversible coagulopathy in elderly patients taking the combination even after suffering blunt head trauma [8, 60].
Omega-3 Fatty Acids and Inflammation
A study conducted by Gutierrez and colleagues showed that omega-3 FA is incorporated throughout the body into the bi-phospholipid layer of the cell membrane of neutrophils and produces different mediators such as prostaglandins, leukotrienes, and maresins. So, if the injury occurs the byproducts of those cell membranes may produce less inflammatory provoking mediators compared to omega-6 FAs, which are more prevalent in the Western diet [58]. Sheppard and colleagues showed that children and adults in the US did not consume sufficient EPA and DHA in their diets. In other terms, Western diets predispose to have a high omega-6/omega-3 ratio which may promote the pathogenesis of many diseases [61, 62]. Further, there is evidence that omega-6 may inhibit the anti-inflammatory effect of omega-3 FAs [63].
Previous studies have been done to clarify the role of omega-3 on anti-inflammatory mechanisms. For example, Saifullah and colleagues carried out a study to know the outcomes of adding EPA and DHA to the diet of hemodialysis patients for 3 months, showing a modest reduction in serum C-reactive protein, which is an inflammatory mediator produced in the liver in response to inflammation [10].
Microorganisms like bacteria, viruses, fungi, protozoa, and worms can all cause infections. Sepsis may occur following infections which can disturb the homeostasis of the body leading to uncontrolled inflammation and ultimately organ failure, shock, and death. A study was done with omega-3 FA lipid emulsion in the cases of sterile peritonitis and murine polymicrobial sepsis demonstrated anti-inflammatory properties of omega-3 FAs. In this study, omega-3 FAs reduced neutrophil infiltration, pro-inflammatory mediators, and classical monocytes while it enhanced non-classical monocyte/macrophage recruitment and efferocytosis in sepsis [64].
Omega-3 FAs include EPA and DHA. Saedisomeolia and colleagues conducted a study to determine the anti-inflammatory properties of DHA and EPA in airway epithelial cells infected with Rhinovirus. In this study, the researchers incubated airway epithelial cells with EPA, DHA, and AA for 24 hours and then infected them with rhinovirus for 48h. They measured IL-6, IL-8, and interferon-gamma-induced protein-10 (IP-10) released by cells using enzyme-linked immunosorbent assay. The investigators found that DHA significantly reduced the release of IL-6 and IP-10 from the cells infected with different strains of rhinovirus. This could be explained by the efficiency of omega-3 FA reducing inflammation by inhibiting AA metabolism to eicosanoids and finally reducing pro-inflammatory cytokines and immune cell function [65].
Omega-3 Fatty Acids and Oxidative Stress
Omega-3 FAs have been found to exhibit antioxidant activity through various mechanisms including upregulating nuclear factor erythroid 2-related factor 2 (NRF2) mediated antioxidant effects, reducing F2 isoprostanes formed during the oxidation of arachidonic acid, inducing PPARγ and modulating toll-like receptor 4 (TLR4) receptors which all lead to a reduction in κβ phosphorylation and thus reduce NF-κβ which in turn reduces inflammatory markers like IL-6, TNFα, and tissue growth factor beta (TGFβ). They also induce mitogen activated protein kinase (MAPK) phosphatases and upregulate glutathione also known as GSH, which is an antioxidant molecule, and upregulate genes responsible for the production of heme-oxygenase, which is cytoprotective. N-3 fatty acids also inhibit lipid peroxidation. They are ultimately metabolized to anti-inflammatory molecules like resolvins, protectins, and maresins [66, 67, 68].
Omega-3 Fatty Acids and Immune System
There is a plethora of ongoing research on the effects of omega-3 FAs and its modifications to the immune system. Omega-3 FAs are considered to be a polyunsaturated fatty acid, which upregulates the activation of immune cells specifically in macrophages, neutrophils, T-cells, B-cells, dendritic cells, natural killer cells, mast cells, basophils, and eosinophils. Omega-3 FA plays a role in the host cellular membrane which regulates membrane fluidity and intricate lipid raft assembling [9]. This is demonstrated in the Figure 2.
Figure 2. How omega-3 fatty acids impact the cellular immune response.Nuclear factor kappa B (NF-κB) is a pro-inflammatory cytokine triggering an inflammatory response via activation of transcription of genes for further pro-inflammatory proteins. Omega-3 fatty acids potentially exert their anti-inflammatory effect via toll-like receptor 4 (TLR4) pathway and G-protein coupled receptor 120 (GPR120) pathway to inhibit the NF-κB and consequently the inflammatory cascade. TAB, TGF-beta activated kinase; TAK, tat-associated kinase; IRAK, interleukin 1 receptor-associated kinase; TRAF6, tumor necrosis factor receptor associated factor 6; TRIAP, TP53 regulated inhibitor of apoptosis; MD2, myeloid differentiation factor 2.
Omega-3 FAs also increase the function of neutrophils which are the first responders of infection in the body. The study showed that omega-3 FAs incorporate phospholipids of the cell membrane of neutrophils and produce different mediators such as prostaglandins, leukotrienes, and maresins. In addition, neutrophils strengthen the immune function by promoting neutrophil migration, phagocytic capacity, and production of reactive free radicals to kill microbes. Omega-3 FAs help activate the function of T cells by promoting antigen-presenting cells (APC), for example, macrophages or dendritic cells. Subsequently, that promotes activation of different subgroups of T cells such as CD4 cells, Th17 cells, and regulatory T cells. B cells are also activated by omega-3 FAs, producing more antibodies utilizing heavy chain immunoglobulin rearrangements and further differentiation. The study claims that omega-3 FAs also increase the population of B cells in the study mice [9]. Omega-3 improves the function of the macrophages by secreting cytokines and chemokines, promoting the ability of phagocytosis, and activating macrophages by polarization [69].
Moreover, the omega-3 FA has appeared to block the activity of NF-κB through decreasing the degradation of the inhibitory subunit of the NF-κB called IkB, in cultured pancreatic cells and human monocyteds. Since NF-κB is responsible for cytokine production in immune cells, by blocking that pathway, its decreasing cytokine storm, and complication [70]. Omega-3 FAs are also known to down-regulate NF-κB. NF-κB is considered to be a transcription factor involved in cell signaling to initiate an inflammatory response by the innate immune system. Furthermore, omega-3 FAs intake upregulates vagal response which in turn down-regulates inflammation and cytokine production. To our understanding omega-3 FAs have multiple effects on the inflammatory response; however, analytic data has not yet recognized its role in critically ill patients. Future research may indicate that supplementation of omega-3 FA fish oils may play a crucial role in SARS-CoV-2 treatment [71].
Omega-3 Fatty Acids and Viral Infection
Omega-3 FAs could be a potential antimicrobial drug with little potential for drug resistance [72]. The metabolites of both omega-3 and omega-6 play an important role in the synthesis of different mediators such as prostaglandins, leukotrienes, thromboxanes, protectins, and resolvins [9]. The study shows that fish oil enhances antiviral response by inducing interferon (IFN) which inhibits viral replication [69]. The anti-inflammatory effect by omega-3 FAs is stronger in DHA compared to that of EPA, and their secretion of cytokines IL-10 is further increased by omega-3. CD8 T cells are responsible for fighting against viruses by inducing the production of different cytokines in the body, such as Tumor Necrosis Factor-alpha (TNF-alpha) and granzyme B. However, the surge of cytokines by CD8 T cells to defend influenza viruses impose unintended lung damage and further deteriorate the clinical outcome. Omega-3 FAs weaken the antiviral response by CD8 T cells and could potentially be used to modulate cytokine responses as antiviral responses, and this process is further explained in Figure 3 [73].
Figure 3. Omega-3 fatty acid acting on different elements of the immune response.Omega-3 fatty acids, through their anti-inflammatory mechanism, inhibit the production of pro-inflammatory mediators like interleukin (IL)-1β, IL-6, tumor necrosis factor (TNF)-α and prevent cytokine storm. Some studies also suggest that they dampen the inflammatory response through regulatory T cells (Treg) differentiation. They also exert an anti-viral effect by enhancing the phagocytic activity of cells of the innate immune system- Neutrophils and Macrophages.
Other Benefits of Omega-3 Fatty Acids
Omega-3 PUFAs include α-linolenic acid (ALA; 18:3 ω-3), stearidonic acid (SDA; 18:4 ω-3), eicosapentaenoic acid (EPA; 20:5 ω-3), docosapentaenoic acid (DPA; 22:5 ω-3), and docosahexaenoic acid (DHA; 22:6 ω-3). The health benefits of omega-3 FA are encompassing and cover a wide range of different organ systems and targets including cardiovascular disease, diabetes, cancer, Alzheimer’s disease, dementia, depression, visual and neurological development, and maternal and child health. Numerous studies have been done that enumerate the reduction in clinical disease rates and mortality rates in patients suffering from a vast array of diseases. Research has been conducted involving humans and omega-3 FA for well over 40 years [74]. Albert and colleagues demonstrated that diets rich in fish and seafood containing high levels of omega-3 PUFAs lead to a statistically significant reduction in mortality from cardiovascular events. The study population included Inuit people who had a diet naturally predominated by seafood and marine life. Men who consumed fish at least once every seven days had a multivariate relative risk of sudden death of 0.48 (95% confidence interval, 0.24 – 0.96; P = 0.04) compared to men who consumed fish less frequently than once per month, demonstrating that diets rich in omega-3’s can reduce the risk of death for men from the cardiovascular event by half [11]. Omega-3 supplementation has also been studied in the setting of ARDS. In a study done in 2015, it was determined that natural antioxidants like omega-3 only lead to a statistically significant decrease in mortality in those suffering from ARDS [75]. Due to the survival rate of COVID-19 patients suffering from ARDS standing at 25%, it is therefore imperative that methods that could potentially provide therapeutic relief or treatment are investigated thoroughly [12]. Although the role of ω-3 supplementation in ARDS needs to be further elucidated, its vital role in reducing reactive oxygen species and pro-inflammatory cytokines, such as TNF-α, IL-1β, IL-6, and IL-8, is widely documented. Therefore, ω-3 PUFAs could be considered for potential interventions for COVID-19 [75].
Omega-3 index, which is the EPA + DHA, is a a percent of total red blood cell fatty acid and is regarded as a new risk factor for death from coronary heart disease (CHD) (Fig. 2). The value of about 8% is estimated to be cardioprotective while that of less than 4% is associated with an increased risk of CHD death [76]. As per our discussion, omega-3 FAs are less prone to the production of different inflammatory markers compared to omega-6 that could initiate a cascade of the cytokine storm. It is evident that the regions with a low index like the USA, few European countries experiencing higher COVID-19 related deaths than those with high index. Omega-3 FAs may play a role in COVID-19 by reducing inflammatory markers and may lower the coronary complications. Figure 4 shows the Global View of Omega-3 Index Levels.
Figure 4. The global view of omega-3 index levels is shown in this figure.The omega-3 index risk zones are as follows: ● High Risk ≤ 4%. ● Intermediate risk = 4 – 8%. ● Low risk > 8%.
Conclusion
There are various benefits of omega-3 FA and taking it as a supplement might be associated with the prevention of the viral entry by changing the composition of fats in the bilipid membrane of cells. Omega-3 FAs, such as DHA and EPA, perform their role by being incorporated in the cell membrane and affecting the clumping of toll-like receptors and thus preventing signals that activate NF-κB and help to ameliorate complications of COVID-19 by producing fewer pro-inflammatory mediators. DHA and EPA are precursors of particles called resolvins D and E, which reduce the proinflammatory mediators thereby reducing pulmonary neutrophils recruitment, increasing apoptosis by macrophages, and subsequently decreasing broncho-alveolar IL-6 production and as a result, decreasing inflammation of the lung. Omega-3 FA plays a role in increasing the phagocytic capacity of macrophages due to the changes in the composition of the cell membrane bilipid layer. Omega-3 FAs also play a role in mediating inflammatory processes and immunomodulation for both innate and acquired immune systems.
It is necessary to understand that the link between omega-3 FA-rich diet and the clinical outcome could be far more complex than previously considered when treating COVID-19 patients. At the very least, this information could serve as the impetus that initiates further conversation and investigation into dietary supplementation that can be considered in both hospitalized patients and patients at home. Several clinical trials are being conducted to investigate the most appropriate treatment for SARS-CoV-2. Due to its anti-inflammatory, immunomodulatory, and other various beneficial properties, omega-3 FA is a natural, inexpensive, and could play a role as a healthier choice of supplement during this ongoing pandemic situation. Future larger randomized blinded clinical trials are warranted and sufficient confirmatory results are required which could further shed light on this topic.
Research shows people with high omega-3 index less likely to die from COVID-19
Pilot study shows positive outcomes for those suffering from COVID-19
Researchers with the Fatty Acid Research Institute (FARI) and collaborators at Cedars-Sinai Medical Center in Los Angeles and in Orange County, CA, have published the first direct evidence that higher omega-3 blood levels may reduce risk for death from COVID-19 infection. The report was published in the journal Prostaglandins, Leukotrienes and Essential Fatty Acids on January 20, 2021.
There are several papers in the medical literature hypothesizing that omega-3 fatty acids should have beneficial effects in patients with COVID-19 infection, but up until now, there have been no published peer-reviewed studies supporting that hypothesis.
This study included 100 patients admitted to the hospital with COVID-19 for whom admission blood samples had been stored. Clinical outcomes for these patients were obtained and blood was analyzed for the Omega-3 Index (O3I, red blood cell membrane EPA+DHA levels) at OmegaQuant Analytics (Sioux Falls, SD). Fourteen of the patients died.
The 100 patients were grouped into four quartiles according to their O3I, with 25% of the patients in each quartile. There was one death in the top quartile (i.e., 1 death out of 25 patients with O3I>5.7%), with 13 deaths in the remaining patients (i.e., 13 deaths out of 75 patients with O3I<5.7%).
In age-and-sex adjusted regression analyses, those in the highest quartile (O3I >5.7%) were 75% less likely to die compared with those in the lower three quartiles (p=0.07). Stated another way, the relative risk for death was about four times higher in those with a lower O3I (<5.7%) compared to those with higher levels.
“While not meeting standard statistical significance thresholds, this pilot study – along with multiple lines of evidence regarding the anti-inflammatory effects of EPA and DHA – strongly suggests that these nutritionally available marine fatty acids may help reduce risk for adverse outcomes in COVID-19 patients. Larger studies are clearly needed to confirm these preliminary findings,” said Arash Asher, MD, the lead author on this study.
Agreeing with Dr. Asher, cardiology researcher and co-developer with Dr. Harris of the Omega-3 Index, Clemens von Schacky, MD, (CEO, Omegametrix GmbH, Martinsried, Germany, and not involved with the study) said, “Asher et al have demonstrated that a low Omega-3 Index might be a powerful predictor for death from COVID-19. Although encouraging, their findings clearly need to be replicated.”
Omega-3 expert James H. O’Keefe, Jr., MD, (Director of Preventive Cardiology, Saint Luke’s Mid America Heart Institute, Kansas City, MO, and also not involved with the study) observed, “An excessive inflammatory response, referred to as a ‘cytokine storm,’ is a fundamental mediator of severe COVID-19 illness. Omega-3 fatty acids (DHA and EPA) have potent anti-inflammatory activities, and this pilot study provides suggestive evidence that these fatty acids may dampen COVID-19’s cytokine storm.”
The FARI research team is currently seeking funding to expand upon these preliminary observations. Individuals and organizations that want to support this research are encouraged to visit FARI’s donations page.
The Fatty Acid Research Institute (FARI) is a non-profit research and education foundation. FARI was founded in order to accelerate discovery of the health effects of fatty acids, most notably, the long chain omega-3 fatty acids EPA and DHA. FARI researchers and scientists will focus single-mindedly on publishing high-quality research studies on the multiple relationships between fatty acid levels and human (and animal) health outcomes. These studies will improve the ability to predict risk for disease, and more importantly, suggest ways to reduce risk by changing our diets and/or supplementation regimens.
ChooseLife Notes:
Again, this builds the picture out, that likelihood of acquiring and gradient of infection are both clearly linked to multiple biological processes, these processes are demonstrably underpinned in many instances, or enhanced greatly in others, by the intelligent adaptation of diet to include plentiful amounts of Omega3, my preference is FlaxOil via Budwig, it adds so many extra facets, partcularly in Mucin production and intestinal fauna well-being (but I am perhaps biased a little as a vegetarian!).
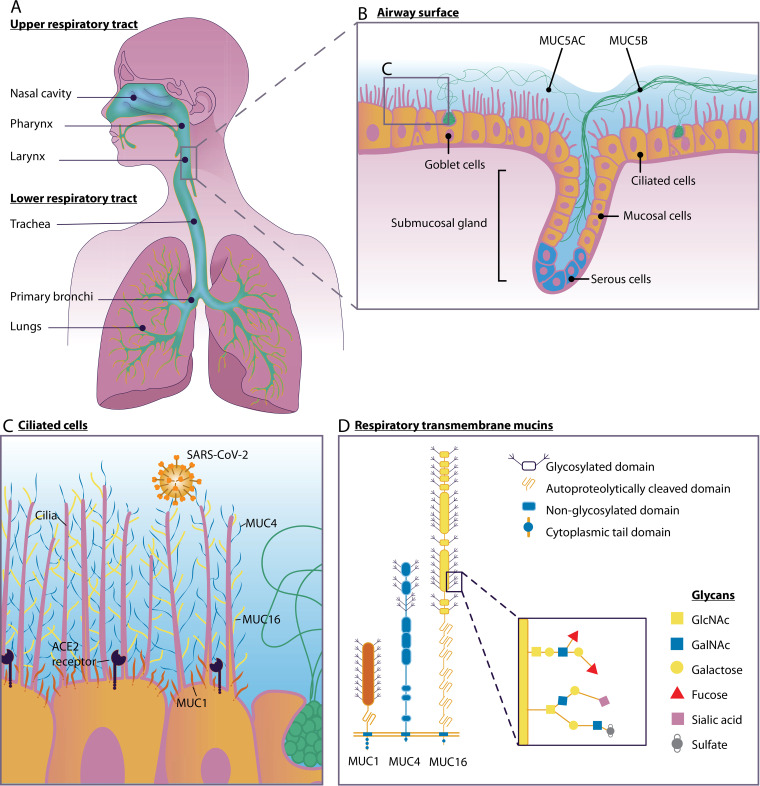
Mucus plays a pivotal role in protecting the respiratory tract against microbial infections. It acts as a primary contact site to entrap microbes and facilitates their removal from the respiratory tract via the coordinated beating of motile cilia. The major components of airway mucus are heavily O-glycosylated mucin glycoproteins, divided into gel-forming mucins and transmembrane mucins. The gel-forming mucins MUC5AC and MUC5B are the primary structural components of airway mucus, and they enable efficient clearance of pathogens by mucociliary clearance. MUC5B is constitutively expressed in the healthy airway, whereas MUC5AC is upregulated in response to inflammatory challenge. MUC1, MUC4, and MUC16 are the three major transmembrane mucins of the respiratory tracts which prevent microbial invasion, can act as releasable decoy receptors, and activate intracellular signal transduction pathways. Pathogens have evolved virulence factors such as adhesins that facilitate interaction with specific mucins and mucin glycans, for example, terminal sialic acids. Mucin expression and glycosylation are dependent on the inflammatory state of the respiratory tract and are directly regulated by proinflammatory cytokines and microbial ligands. Gender and age also impact mucin glycosylation and expression through the female sex hormone estradiol and age-related downregulation of mucin production. Here, we discuss what is currently known about the role of respiratory mucins and their glycans during bacterial and viral infections of the airways and their relevance for the novel coronavirus severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Understanding the impact of microbe-mucin interaction in the respiratory tract could inspire the development of novel therapies to boost mucosal defense and combat respiratory infections.
Mucosal defense in the respiratory tract during SARS-CoV-2 infection. (A) Human upper and lower respiratory tracts. (B) Respiratory epithelium with ciliated cells, goblet cells, and a submucosal gland. The soluble mucin MUC5AC is secreted by goblet cells, and the soluble mucin MUC5B is secreted by mucosal cells in the submucosal gland. (C) Ciliated epithelial cells express transmembrane mucins MUC1 (red), MUC4 (blue), and MUC16 (yellow) and the SARS-CoV-2 entry receptor ACE2. (D) Domain structure of transmembrane mucins MUC1, MUC4, and MUC16. Mucin O-glycan structures and, specifically, terminal sialic acids play an important role in virus-mucin interactions.
We, doctors and health professionals, wish to express our serious concern about the evolution of the situation in the recent months surrounding the outbreak of the SARS-CoV-2 virus. We call on politicians to be independently and critically informed in the decision-making process and in the compulsory implementation of corona-measures. We ask for an open debate, where all experts are represented without any form of censorship. After the initial panic surrounding covid-19, the objective facts now show a completely different picture – there is no medical justification for any emergency policy anymore. The current crisis management has become totally disproportionate and causes more damage than it does any good. We call for an end to all measures and ask for an immediate restoration of our normal democratic governance and legal structures and of all our civil liberties.
‘A cure must not be worse than the problem’ is a thesis that is more relevant than ever in the current situation. We note, however, that the collateral damage now being caused to the population will have a greater impact in the short and long term on all sections of the population than the number of people now being safeguarded from corona. In our opinion, the current corona measures and the strict penalties for non-compliance with them are contrary to the values formulated by the Belgian Supreme Health Council, which, until recently, as the health authority, has always ensured quality medicine in our country: “Science – Expertise – Quality – Impartiality – Independence – Transparency”. 1
We believe that the policy has introduced mandatory measures that are not sufficiently scientifically based, unilaterally directed, and that there is not enough space in the media for an open debate in which different views and opinions are heard. In addition, each municipality and province now has the authorisation to add its own measures, whether well-founded or not.
Moreover, the strict repressive policy on corona strongly contrasts with the government’s minimal policy when it comes to disease prevention, strengthening our own immune system through a healthy lifestyle, optimal care with attention for the individual and investment in care personnel.2
The concept of health
In 1948, the WHO defined health as follows: ‘Health is a state of complete physical, mental and social well-being and not merely the absence of disease or other physical impairment’.3
Health, therefore, is a broad concept that goes beyond the physical and also relates to the emotional and social well-being of the individual. Belgium also has a duty, from the point of view of subscribing to fundamental human rights, to include these human rights in its decision-making when it comes to measures taken in the context of public health. 4 The current global measures taken to combat SARS-CoV-2 violate to a large extent this view of health and human rights. Measures include compulsory wearing of a mask (also in open air and during sporting activities, and in some municipalities even when there are no other people in the vicinity), physical distancing, social isolation, compulsory quarantine for some groups and hygiene measures.
The predicted pandemic with millions of deaths
At the beginning of the pandemic, the measures were understandable and widely supported, even if there were differences in implementation in the countries around us. The WHO originally reported in March that the death rate among the registered covid-19 cases was 3.4%. Millions of deaths were thus foreseen, and an extremely contagious virus for which no treatment or vaccine was available. This would put unprecedented pressure on the intensive care units (ICUs) of our hospitals.
This led to a global alarm situation, never seen in the history of mankind: “flatten the curve” was represented by a lockdown that shut down the entire society and economy and quarantined healthy people. Social distancing became the new normal in anticipation of a rescue vaccine.
The facts about covid-19
Gradually, the alarm bell was sounded from many sources: the objective facts showed a completely different reality. 56
The course of covid-19 followed the course of a normal wave of infection similar to a flu season. As every year, we see a mix of flu viruses following the curve: first the rhinoviruses, then the influenza A and B viruses, followed by the coronaviruses. There is nothing different from what we normally see.
The use of the non-specific PCR test, which produces many false positives, showed an exponential picture. This test was rushed through with an emergency procedure and was never seriously self-tested. The creator expressly warned that this test was intended for research and not for diagnostics.7 The PCR test works with cycles of amplification of genetic material – a piece of genome is amplified each time. Any contamination (e.g. other viruses, debris from old virus genomes) can possibly result in false positives.8
The test does not measure how many viruses are present in the sample. A real viral infection means a massive presence of viruses, the so-called virus load. If someone tests positive, this does not mean that that person is actually clinically infected, is ill or is going to become ill. Koch’s postulate was not fulfilled (“The pure agent found in a patient with complaints can provoke the same complaints in a healthy person”).
Since a positive PCR test does not automatically indicate active infection or infectivity, this does not justify the social measures taken, which are based solely on these tests. 910
Lockdown.
If we compare the waves of infection in countries with strict lockdown policies to countries that did not impose lockdowns (Sweden, Iceland …), we see similar curves. So there is no link between the imposed lockdown and the course of the infection. Lockdown has not led to a lower mortality rate.
If we look at the date of application of the imposed lockdowns we see that the lockdowns were set after the peak of the virus replication rate was already over and decreasing. The drop was therefore not the result of the taken measures. 11 As every year, it seems that climatic conditions (weather, temperature and humidity) and growing immunity are more likely to reduce the wave of infection.
Our immune system
For thousands of years, the human body has been exposed daily to moisture and droplets containing infectious microorganisms (viruses, bacteria and fungi).
The penetration of these microorganisms is prevented by an advanced defence mechanism – the immune system. A strong immune system relies on normal daily exposure to these microbial influences. Overly hygienic measures have a detrimental effect on our immunity. 1213 Only people with a weak or faulty immune system should be protected by extensive hygiene or social distancing.
Influenza will re-emerge in the autumn (in combination with covid-19) and a possible decrease in natural resilience may lead to further casualties.
Our immune system consists of two parts: a congenital, non-specific immune system and an adaptive immune system.
The non-specific immune system forms a first barrier: skin, saliva, gastric juice, intestinal mucus, vibratory hair cells, commensal flora, … and prevents the attachment of micro-organisms to tissue.
If they do attach, macrophages can cause the microorganisms to be encapsulated and destroyed.
The adaptive immune system consists of mucosal immunity (IgA antibodies, mainly produced by cells in the intestines and lung epithelium), cellular immunity (T-cell activation), which can be generated in contact with foreign substances or microorganisms, and humoral immunity (IgM and IgG antibodies produced by the B cells).
Recent research shows that both systems are highly entangled.
It appears that most people already have a congenital or general immunity to e.g. influenza and other viruses. This is confirmed by the findings on the cruise ship Diamond Princess, which was quarantined because of a few passengers who died of Covid-19. Most of the passengers were elderly and were in an ideal situation of transmission on the ship. However, 75% did not appear to be infected. So even in this high-risk group, the majority are resistant to the virus.
A study in the journal Cell shows that most people neutralise the coronavirus by mucosal (IgA) and cellular immunity (T-cells), while experiencing few or no symptoms 14.
Researchers found up to 60% SARS-Cov-2 reactivity with CD4+T cells in a non-infected population, suggesting cross-reactivity with other cold (corona) viruses.15
Most people therefore already have a congenital or cross-immunity because they were already in contact with variants of the same virus.
The antibody formation (IgM and IgG) by B-cells only occupies a relatively small part of our immune system. This may explain why, with an antibody percentage of 5-10%, there may be a group immunity anyway. The efficacy of vaccines is assessed precisely on the basis of whether or not we have these antibodies. This is a misrepresentation.
Most people who test positive (PCR) have no complaints. Their immune system is strong enough. Strengthening natural immunity is a much more logical approach. Prevention is an important, insufficiently highlighted pillar: healthy, full-fledged nutrition, exercise in fresh air, without a mask, stress reduction and nourishing emotional and social contacts.
Consequences of social isolation on physical and mental health
Social isolation and economic damage led to an increase in depression, anxiety, suicides, intra-family violence and child abuse.16
Studies have shown that the more social and emotional commitments people have, the more resistant they are to viruses. It is much more likely that isolation and quarantine have fatal consequences. 17
The isolation measures have also led to physical inactivity in many older people due to their being forced to stay indoors. However, sufficient exercise has a positive effect on cognitive functioning, reducing depressive complaints and anxiety and improving physical health, energy levels, well-being and, in general, quality of life.18
Fear, persistent stress and loneliness induced by social distancing have a proven negative influence on psychological and general health. 19
A highly contagious virus with millions of deaths without any treatment?
Mortality turned out to be many times lower than expected and close to that of a normal seasonal flu (0.1-0.5%). 20 The number of registered corona deaths therefore still seems to be overestimated. There is a difference between death by corona and death with corona. Humans are often carriers of multiple viruses and potentially pathogenic bacteria at the same time. Taking into account the fact that most people who developed serious symptoms suffered from additional pathology, one cannot simply conclude that the corona-infection was the cause of death. This was mostly not taken into account in the statistics.
The most vulnerable groups can be clearly identified. The vast majority of deceased patients were 80 years of age or older. The majority (70%) of the deceased, younger than 70 years, had an underlying disorder, such as cardiovascular suffering, diabetes mellitus, chronic lung disease or obesity. The vast majority of infected persons (>98%) did not or hardly became ill or recovered spontaneously.
Meanwhile, there is an affordable, safe and efficient therapy available for those who do show severe symptoms of disease in the form of HCQ (hydroxychloroquine), zinc and azithromycin. Rapidly applied this therapy leads to recovery and often prevents hospitalisation. Hardly anyone has to die now.
This effective therapy has been confirmed by the clinical experience of colleagues in the field with impressive results. This contrasts sharply with the theoretical criticism (insufficient substantiation by double-blind studies) which in some countries (e.g. the Netherlands) has even led to a ban on this therapy. A meta-analysis in The Lancet, which could not demonstrate an effect of HCQ, was withdrawn. The primary data sources used proved to be unreliable and 2 out of 3 authors were in conflict of interest. However, most of the guidelines based on this study remained unchanged … 4849 We have serious questions about this state of affairs. In the US, a group of doctors in the field, who see patients on a daily basis, united in “America’s Frontline Doctors” and gave a press conference which has been watched millions of times.2151 French Prof Didier Raoult of the Institut d’Infectiologie de Marseille (IHU) also presented this promising combination therapy as early as April. Dutch GP Rob Elens, who cured many patients in his practice with HCQ and zinc, called on colleagues in a petition for freedom of therapy.22 The definitive evidence comes from the epidemiological follow-up in Switzerland: mortality rates compared with and without this therapy.23
From the distressing media images of ARDS (acute respiratory distress syndrome) where people were suffocating and given artificial respiration in agony, we now know that this was caused by an exaggerated immune response with intravascular coagulation in the pulmonary blood vessels. The administration of blood thinners and dexamethasone and the avoidance of artificial ventilation, which was found to cause additional damage to lung tissue, means that this dreaded complication, too, is virtually not fatal anymore. 47
It is therefore not a killer virus, but a well-treatable condition.
Propagation
Spreading occurs by drip infection (only for patients who cough or sneeze) and aerosols in closed, unventilated rooms. Contamination is therefore not possible in the open air. Contact tracing and epidemiological studies show that healthy people (or positively tested asymptomatic carriers) are virtually unable to transmit the virus. Healthy people therefore do not put each other at risk. 2425 Transfer via objects (e.g. money, shopping or shopping trolleys) has not been scientifically proven.262728
All this seriously calls into question the whole policy of social distancing and compulsory mouth masks for healthy people – there is no scientific basis for this.
Masks
Oral masks belong in contexts where contacts with proven at-risk groups or people with upper respiratory complaints take place, and in a medical context/hospital-retirement home setting. They reduce the risk of droplet infection by sneezing or coughing. Oral masks in healthy individuals are ineffective against the spread of viral infections. 293031
Wearing a mask is not without side effects. 3233Oxygen deficiency (headache, nausea, fatigue, loss of concentration) occurs fairly quickly, an effect similar to altitude sickness. Every day we now see patients complaining of headaches, sinus problems, respiratory problems and hyperventilation due to wearing masks. In addition, the accumulated CO2 leads to a toxic acidification of the organism which affects our immunity. Some experts even warn of an increased transmission of the virus in case of inappropriate use of the mask.34
Our Labour Code (Codex 6) refers to a CO2 content (ventilation in workplaces) of 900 ppm, maximum 1200 ppm in special circumstances. After wearing a mask for one minute, this toxic limit is considerably exceeded to values that are three to four times higher than these maximum values. Anyone who wears a mask is therefore in an extreme poorly ventilated room. 35
Inappropriate use of masks without a comprehensive medical cardio-pulmonary test file is therefore not recommended by recognised safety specialists for workers. Hospitals have a sterile environment in their operating rooms where staff wear masks and there is precise regulation of humidity / temperature with appropriately monitored oxygen flow to compensate for this, thus meeting strict safety standards. 36
A second corona wave?
A second wave is now being discussed in Belgium, with a further tightening of the measures as a result. However, closer examination of Sciensano’s figures37 shows that, although there has been an increase in the number of infections since mid-July, there was no increase in hospital admissions or deaths at that time. It is therefore not a second wave of corona, but a so-called “case chemistry” due to an increased number of tests. 50 The number of hospital admissions or deaths showed a shortlasting minimal increase in recent weeks, but in interpreting it, we must take into account the recent heatwave. In addition, the vast majority of the victims are still in the population group >75 years. This indicates that the proportion of the measures taken in relation to the working population and young people is disproportionate to the intended objectives. The vast majority of the positively tested “infected” persons are in the age group of the active population, which does not develop any or merely limited symptoms, due to a well-functioning immune system. So nothing has changed – the peak is over.
Strengthening a prevention policy
The corona measures form a striking contrast to the minimal policy pursued by the government until now, when it comes to well-founded measures with proven health benefits such as the sugar tax, the ban on (e-)cigarettes and making healthy food, exercise and social support networks financially attractive and widely accessible. It is a missed opportunity for a better prevention policy that could have brought about a change in mentality in all sections of the population with clear results in terms of public health. At present, only 3% of the health care budget goes to prevention. 2
The Hippocratic Oath
As a doctor, we took the Hippocratic Oath: “I will above all care for my patients, promote their health and alleviate their suffering”.
“I will inform my patients correctly.”
“Even under pressure, I will not use my medical knowledge for practices that are against humanity.” The current measures force us to act against this oath. Other health professionals have a similar code.
The ‘primum non nocere’, which every doctor and health professional assumes, is also undermined by the current measures and by the prospect of the possible introduction of a generalised vaccine, which is not subject to extensive prior testing.
Vaccine
Survey studies on influenza vaccinations show that in 10 years we have only succeeded three times in developing a vaccine with an efficiency rate of more than 50%. Vaccinating our elderly appears to be inefficient. Over 75 years of age, the efficacy is almost non-existent.38 Due to the continuous natural mutation of viruses, as we also see every year in the case of the influenza virus, a vaccine is at most a temporary solution, which requires new vaccines each time afterwards. An untested vaccine, which is implemented by emergency procedure and for which the manufacturers have already obtained legal immunity from possible harm, raises serious questions. 3940 We do not wish to use our patients as guinea pigs. On a global scale, 700 000 cases of damage or death are expected as a result of the vaccine.41 If 95% of people experience Covid-19 virtually symptom-free, the risk of exposure to an untested vaccine is irresponsible.
The role of the media and the official communication plan
Over the past few months, newspaper, radio and TV makers seemed to stand almost uncritically behind the panel of experts and the government, there, where it is precisely the press that should be critical and prevent one-sided governmental communication. This has led to a public communication in our news media, that was more like propaganda than objective reporting.
In our opinion, it is the task of journalism to bring news as objectively and neutrally as possible, aimed at finding the truth and critically controlling power, with dissenting experts also being given a forum in which to express themselves.
This view is supported by the journalistic codes of ethics.42
The official story that a lockdown was necessary, that this was the only possible solution, and that everyone stood behind this lockdown, made it difficult for people with a different view, as well as experts, to express a different opinion.
Alternative opinions were ignored or ridiculed. We have not seen open debates in the media, where different views could be expressed.
We were also surprised by the many videos and articles by many scientific experts and authorities, which were and are still being removed from social media. We feel that this does not fit in with a free, democratic constitutional state, all the more so as it leads to tunnel vision. This policy also has a paralysing effect and feeds fear and concern in society. In this context, we reject the intention of censorship of dissidents in the European Union! 43
The way in which Covid-19 has been portrayed by politicians and the media has not done the situation any good either. War terms were popular and warlike language was not lacking. There has often been mention of a ‘war’ with an ‘invisible enemy’ who has to be ‘defeated’. The use in the media of phrases such as ‘care heroes in the front line’ and ‘corona victims’ has further fuelled fear, as has the idea that we are globally dealing with a ‘killer virus’.
The relentless bombardment with figures, that were unleashed on the population day after day, hour after hour, without interpreting those figures, without comparing them to flu deaths in other years, without comparing them to deaths from other causes, has induced a real psychosis of fear in the population. This is not information, this is manipulation.
We deplore the role of the WHO in this, which has called for the infodemic (i.e. all divergent opinions from the official discourse, including by experts with different views) to be silenced by an unprecedented media censorship.4344
We urgently call on the media to take their responsibilities here!
We demand an open debate in which all experts are heard.
Emergency law versus Human Rights
The general principle of good governance calls for the proportionality of government decisions to be weighed up in the light of the Higher Legal Standards: any interference by government must comply with the fundamental rights as protected in the European Convention on Human Rights (ECHR). Interference by public authorities is only permitted in crisis situations. In other words, discretionary decisions must be proportionate to an absolute necessity.
The measures currently taken concern interference in the exercise of, among other things, the right to respect of private and family life, freedom of thought, conscience and religion, freedom of expression and freedom of assembly and association, the right to education, etc., and must therefore comply with fundamental rights as protected by the European Convention on Human Rights (ECHR). For example, in accordance with Article 8(2) of the ECHR, interference with the right to private and family life is permissible only if the measures are necessary in the interests of national security, public safety, the economic well-being of the country, the protection of public order and the prevention of criminal offences, the protection of health or the protection of the rights and freedoms of others, the regulatory text on which the interference is based must be sufficiently clear, foreseeable and proportionate to the objectives pursued.45
The predicted pandemic of millions of deaths seemed to respond to these crisis conditions, leading to the establishment of an emergency government. Now that the objective facts show something completely different, the condition of inability to act otherwise (no time to evaluate thoroughly if there is an emergency) is no longer in place. Covid-19 is not a killervirus, but a well treatable condition with a mortality rate comparable to the seasonal flu. In other words, there is no longer an insurmountable obstacle to public health.
There is no state of emergency.
Immense damage caused by the current policies
An open discussion on corona measures means that, in addition to the years of life gained by corona patients, we must also take into account other factors affecting the health of the entire population. These include damage in the psychosocial domain (increase in depression, anxiety, suicides, intra-family violence and child abuse)16 and economic damage.
If we take this collateral damage into account, the current policy is out of all proportion, the proverbial use of a sledgehammer to crack a nut.
We find it shocking that the government is invoking health as a reason for the emergency law.
As doctors and health professionals, in the face of a virus which, in terms of its harmfulness, mortality and transmissibility, approaches the seasonal influenza, we can only reject these extremely disproportionate measures.
We therefore demand an immediate end to all measures.
We are questioning the legitimacy of the current advisory experts, who meet behind closed doors.
Following on from ACU 2020 46https://acu2020.org/nederlandse-versie/ we call for an in-depth examination of the role of the WHO and the possible influence of conflicts of interest in this organisation. It was also at the heart of the fight against the “infodemic”, i.e. the systematic censorship of all dissenting opinions in the media. This is unacceptable for a democratic state governed by the rule of law.43
Distribution of this letter
We would like to make a public appeal to our professional associations and fellow carers to give their opinion on the current measures.
We draw attention to and call for an open discussion in which carers can and dare to speak out.
With this open letter, we send out the signal that progress on the same footing does more harm than good, and call on politicians to inform themselves independently and critically about the available evidence – including that from experts with different views, as long as it is based on sound science – when rolling out a policy, with the aim of promoting optimum health.
This letter was originally intended for Belgian doctors and health professionals/Belgian citizens.
More and more foreign colleagues reacted as well and wanted to sign the open letter. The objectively substantiated facts and our demand for an immediate end to all further measures appear to have crossed all borders. We decided therefore at one point to definitively open the letter to all doctors – anywhere in the world – who agree with its content.
This way, the open letter becomes an internationally supported document that aims to openly expose the fake pandemic, which is being perpetuated by the media and governments all over the world.With concern, hope and in a personal capacity.
Lambrecht, B., Hammad, H. The immunology of the allergy epidemic and the hygiene hypothesis. Nat Immunol 18, 1076–1083 (2017). https://www.nature.com/articles/ni.3829
Sharvan Sehrawat, Barry T. Rouse, Does the hygiene hypothesis apply to COVID-19 susceptibility?, Microbes and Infection, 2020, ISSN 1286-4579, https://doi.org/10.1016/j.micinf.2020.07.002
Feys, F., Brokken, S., & De Peuter, S. (2020, May 22). Risk-benefit and cost-utility analysis for COVID-19 lockdown in Belgium: the impact on mental health and wellbeing. https://psyarxiv.com/xczb3/
Haralambieva, I.H. et al., 2015. The impact of immunosenescence on humoral immune response variation after influenza A/H1N1 vaccination in older subjects. https://pubmed.ncbi.nlm.nih.gov/26044074/
The current coronavirus disease 2019 (COVID-19) pandemic presents a global challenge for managing acutely ill patients and complications from viral infection. Systemic inflammation accompanied by a “cytokine storm,” hemostasis alterations and severe vasculitis have all been reported to occur with COVID-19, and emerging evidence suggests that dysregulation of lipid transport may contribute to some of these complications. Here, we aim to summarize the current understanding of the potential mechanisms related to COVID-19 dyslipidemia and propose possible adjunctive type therapeutic approaches that modulate lipids and lipoproteins. Specifically, we hypothesize that changes in the quantity and composition of high-density lipoprotein (HDL) that occurs with COVID-19 can significantly decrease the anti-inflammatory and anti-oxidative functions of HDL and could contribute to pulmonary inflammation. Furthermore, we propose that lipoproteins with oxidized phospholipids and fatty acids could lead to virus-associated organ damage via overactivation of innate immune scavenger receptors. Restoring lipoprotein function with ApoA-I raising agents or blocking relevant scavenger receptors with neutralizing antibodies could, therefore, be of value in the treatment of COVID-19. Finally, we discuss the role of omega-3 fatty acids transported by lipoproteins in generating specialized proresolving mediators and how together with anti-inflammatory drugs, they could decrease inflammation and thrombotic complications associated with COVID-19.
JOURNAL OF BIOLOGICAL REGULATORS & HOMEOSTATIC AGENTS
Vol. 34, no. 4, xx-xx (2020) – Received May 13, 2020 – Accepted June 9, 2020
M. Fioranelli¹, A. Sepehri¹, M.G. Roccia¹,
M. Jafferany²,
O. Yu. Olisova³, K.M. Lomonosov³ and T. Lotti¹,³
¹Department of Nuclear, Sub-nuclear and Radiation Physics, G. MarconiUniversity, Rome, Italy;
²Central Michigan Saginaw, Michigan , USA;
³Department of Dermatology and Venereology, I.M.Sechenov First Moscow State Medical University, Moscow, Russia
In this research, we show that 5G millimeter waves could be absorbed by dermatologic cells acting like antennas, transferred to other cells and play the main role in producing Coronaviruses in biological cells. DNA is built from charged electrons and atoms and has an inductor-like structure. This structure could be divided into linear, toroid and round inductors. Inductors interact with external electromagnetic waves, move and produce some extra waves within the cells. The shapes of these waves are similar to shapes of hexagonal and pentagonal bases of their DNA source. These waves produce some holes in liquids within the nucleus. To fill these holes, some extra hexagonal andpentagonal bases are produced. These bases could join to each other and form virus-like structures such as Coronavirus. To produce these viruses within a cell, it is necessary that the wavelength of external waves be shorter than the size of the cell. Thus 5G millimeter waves could be good candidates for applying in constructing virus-like structures such as Coronaviruses (COVID-19) within cells.
Coronavirus disease (COVID-19) is the main problem this year involving the entire world (1). This is an infectious disease caused by a newly-discovered coronavirus. This virus is a member of related viruses that cause diseases in mammals and birds. In humans, coronaviruses cause respiratory tract infections that can be mild, such as some cases of the common cold (among other possible causes, predominantly rhinoviruses), and others that can be lethal, such as SARS, MERS, and COVID-19. Among them, COVID-19 is an enveloped virus with a positive-sense single-stranded RNA genome and anucleocapsid of helical symmetry. The genome size of coronaviruses ranges from approximately 27 to 34 kilo bases, the largest among known RNA viruses (2, 3).
To date, many scientists have tried to find a method to cure this disease (4, 5); however, without success. COVID-19 may have effects on different types of cells. For example, it has been argued that this virus may have some effects on dermatologic cells (6). On the other hand, it has been known that some waves in 5G technology have direct effects on the skin cells (7). Thus, there are some similarities between effects of COVID-19 and waves in 5G technology.
A new question arises regarding a relationship between 5G technology and COVID-19. The 5G technology is the fifth-generation mobile technology in which its frequency spectrum could be divided into millimeter waves, mid-band, and low-band. Low- band uses a similar frequency range as the predecessor, 4G. 5G millimeter wave is the fastest, with actual speeds often being 1–2 Gbit/s down. Its frequencies are above 24 GHz, reaching up to 72 GHz, which is above the extremely high frequency band’s lower boundary. Millimeter waves have shorter range than microwaves, therefore the reactive cells are those with smaller size (8-10). Consequently, biological cells also could act like a receiver for these waves. Many researchers have considered the effects of 5G technology on human health. For example, it has been shown that 5G mobile networking technology will affect not only the skin and eyes, but will have adverse systemic effects as well (11). In another study, it was argued that 5G technologies cause great harm to human health. Cancer is only one of the many problems. 5G causes 720 (factorial) different diseases in human beings, and can kill everything that lives except some forms of microorganisms (12). To consider the effects of 5G millimeter waves on biological systems, we propose a model which describes the process of exchanging waves between 5G towers and host cells.
To date, some researchers have tried to propose a model for using waves in extracting information within cells (13, 14). These waves could be transverse electromagnetic fields or longitudinal ultrasound waves. A DNA is built from charged particles and according to laws of physics, by any motion of these particles, some electromagnetic waves emerge(15). Also, the structure of a DNA is similar to the structure of an inductor (16) in a receiver and can produce some waves. Thus, a DNA could emit some waves and interact with external waves. However, most waves have a length more than the size of cells and pass them without any effect. Only limited waves with lengths smaller than millimeter could penetrate into cell membrane and interact with DNA inductors. These wavelengths could be observed in 5G technology. Thus, towers in this technology could exchange waves with DNAs within cells and produce various types of diseases such as COVID-19. In this study, we propose a mechanism for exchanged waves between towers and host cells to obtain effective wavelengths. In our method, skin cells act as dermatologic antenna, take waves in 5G technology and transfer them to host cells. Then, DNAs within host cells interact with these waves and move. By motions of a DNA, some hexagonal and pentagonal holes emerge. To fill these holes,some bases are constructed within cells. These holes join to each other and form RNAs of COVID-19.
MATERIALS AND METHODS
A mechanism for exchanging waves between towers and dermatologic cells in 5G technology.
Skin cells are in close connections with nerve fibers. These fibers in the nervous system play the role of wires which carry some electrical currents; these currents produce some electromagnetic waves. These waves and currents are taken by melanocytes, keratinocytes and other dermatologic cells and transmitted to the medium. On the other hand, skin cells could take waves of towers and transfer to other cells and neurons. Thus, dermatologic cells could act as an antenna (Fig. 1).
An antenna could take waves in which their wavelengths are equal to its size. Thus, millimeter waves in 5G technology could be taken more by dermatologic antennas. These waves could pass the cell membranes,enter the nucleus and interact with DNAs. Previously, it has been shown that a DNA could act as the inductor and receiver or sender of waves (16). Thus, a DNA within a dermatologic cell like a keratinocyte receives external waves and sends them to DNAs of other cells like melanocytes. Waves in 5G technology and higher technologies could contribute in gene expressions, turn on some genes and turn off others (Fig. 2).
The question is whether millimeter waves in 5G technology could contribute in constructing some viruses like COVID-19 within a cell. To reply to this question, we should consider the electronic structure of a DNA and its emitted waves. A DNA is built from atoms and electrons. These particles have some electrical charges and emit electrical fields. Also, by each motion of a DNA, its atoms and electrons move. According to the laws of physics, by motion of charged particles, some magnetic waves emerge. Consequently, a DNA emits both electrical and magnetic fields and plays the role of electrical devices within a cell. The structure of a DNA within a cell is similar to the structure of an inductor. When a DNA coils around a nucleosome, it takes the shape of a toroid inductor. Also, by coiling around another axes, a DNA becomes very similar to round inductors (Fig. 3).
Fig. 1. Some waves in 5G technology could be taken by dermatologic antennas, however radio waves could not pass the skin cells
Fig. 2. Waves in 5G technology pass the cell membranes and contribute to gene expressions
Fig. 3. A similarity between different states of DNA with different types of inductors
A DNA coils several times around different axes within chromosomes and produces different types of inductors and electronic devices. Thus, any state of a DNA is similar to a type of an inductor and emits a special wave. Some of these waves are linear, some are curved and others have toroidal shapes (Fig. 4).
A DNA, as an electronic device within a cell, could exchange waves with medium, especially when an electromagnetic wave passes the cell membrane and the nuclear membrane, it induces an extra magnetic field within the DNA inductor and interacts with its fields. This interaction causes extra motions of this DNA, and through the motion of this DNA, its charges move and emit electromagnetic waves. The wavelength of emitted waves from a DNA is equal or less than its size within a cell. Also, shapes of radiated waves by a DNA have direct relations with the shapes of their genetic source. A DNA is formed from hexagonal and pentagonal manifolds; thus,its emitted waves have hexagonal and pentagonal shapes. These waves produce hexagonal and pentagonal holes within the liquids of a nucleus and a cell. To fill these holes, hexagonal and pentagonal molecules are built. These extra hexagonal and pentagonal bases may join to each other and form structures like RNAs of COVID-19 viruses. To produce these viruses, it is necessary that the wave lengths of external electromagnetic fields be equal or less than the size of a cell. For this reason, 5G technology waves could have the main role in the emergence of COVID-19, however radio waves could not have any effect on the evolutions within a cell (Fig. 5).
RESULTS
Effective wavelengths within a cell in 5G technology We propose a model to obtain a probability for the amount of effects of external fields on the evolutions of cells within a cell. This probability is related to the number of micro states of a DNA within a cell:PDNA = ΩDNA, EM / ΩDNA, tot (1)
Where ΩDNA is the probability, ΩDNA, EM is the number of micro states which are produced by the interaction between DNAs and electromagnetic waves, and ΩDNA, tot is the total number of micro states. These micro states have direct relations with entropies:
SDNA = KS LOG (ΩDNA, EM) (2)
Where SDNA is the entropy and KS is a constant. On the other hand, entropies have direct relations with energies:
SDNA =EDNA / Tcell (3)
Where EDNA is the excited energy of a DNA and Tcell is the temperature within a cell. Excited energy of a DNA depends on the linear and curved energies of hexagonal and pentagonal bases:
EDNA = UB, linear,5 V B, linear,5 + UB, curved,5 V B, curved,5 + UB, supercoil,5 V B, supercoil,5 + UB, linear,6 V B, linear,6 + UB, curved,6 V B, curved,6 + UB, supercoil,6 V B, supercoil,6 (4)
Fig. 4. A DNA within the nucleus acts as the inductor and emits magnetic waves
Where UB, linear,5/6 is the energy density of a pentagonal/hexagonal molecule, V B, linear, ,5/6 is the volume of a pentagonal/hexagonal disk , UB, curved, ,5/6 is the energy density of a pentagonal/hexagonal molecule which coils around a nucleosome, V B, curved, ,5/6 is the volume of a coiled pentagonal/hexagonal disk, UB, supercoil, ,5/6 is the energy density of a pentagonal/hexagonal molecule which coils around supercoil axes and V B, supercoil, ,5/6 is its volume. Volumes can be obtained from the following equations:
V B, linear,5 = 5 [1/2 (rbase + xEM )2 cos (ϴpenta)sin(ϴpenta)][ rbase + xEM] V B, linear,6 = 5 [1/2 (rbase + xEM )2 cos (ϴhexa)sin(ϴhexa)] [ rbase + xEM] V B, curved,5 = 5π [1/2 (rbase + xEM )2 cos (ϴpenta) sin(ϴpenta)]× [ rbase + xEM][ rhistone + xEM]2 V B, curved,6 = 5π [1/2 (rbase + xEM )2 cos (ϴhexa)sin(ϴhexa)] )]× [ rbase + xEM][ rhistone + xEM]2
Fig. 5. 5G technology waves could pass the cell membranes and lead to production of COVID-19; however the size of radio waves are more than the size of cells and thus radio waves could not pass the cell membranes.
Where rbase is the length of a base (~10-9), rhistone is the radius of histones (~10-8), rsupercoil is the radius of a supercoil (~ 10-7), ϴhexa (π/6) is the central angle of a hexagonal molecule, ϴpenta (π/5) is the central angle of pentagonal molecule, xEM is the oscillating length which has a direct relation with the wavelength of external field:
EEM =1/2 KEM xEM 2 = h υEM = h c/ λEM (6)
Where υEM is the frequency, λEM is the wavelength of external field, c is the velocity of light and h is the plank constant. Thus, we can write the following equation: xEM ~ λEM -1/2 (7)
We should then calculate magnetic energies and magnetic fields. We assume that a DNA acts like an inductor and thus, we write the following equation for its magnetic fields: For linear inductor:
Where ngene5/6 is the density of genes including hexagonal and pentagonal molecules (17) within DNAs, rhistone is the size of histone (3 × 10-10) (18), rsupercoil is the radius of supercoil (~ 10-9) and Igene,5/6 is there current which moves along pentagonal/hexagonal molecules of genes. We assume that each gene is in fact a long wire that is coiled around the axis of a DNA. A DNA may have 50,000 or more gene (Ngene) (17) and each gene is around 10-12 meter long (Lgene) within a cell. Thus, we can calculate density of genes (ngene):
To calculate the value of the current along genes, we should calculate the total effective charge of all genes (Qgene,5/6) and their velocity (Vgene,5/6). Igene,5/6 = Qgene,5/6 Vgene,5/6 (16) Effective charges of all genes are different from their normal total charges. A gene may have a few normal charges because its charges cancel the effect of each other in the static state. However, during the gene expression and DNA evolutions, each charge has a separate effect. For this reason, we should regard total charges of all genes. To obtain this charge, we should write:
Qgene,5/6 = Ngene,5/6 qgene,5/6 (17)
Where Ngene,5/6 =2 Ngene is the number of genes including pentagonal/hexagonal molecules and qgene,5/6 is the effective charge of pentagonal/hexagonal molecules in a gene. Again, we insist that effective charge of a gene is different from its normal charge. In fact, we should regard all electrons and atoms that contribute in gene expression. For this reason, we should write:
qgene,5/6 =4Nbase qbase (18)
where Nbase is the number of base pairs within a gene (17, 18) and qbase is the effective electrical charge of a base. We can put approximate numbers and obtain the effective charge of all genes:
Now, we calculate the effective velocity of genes:
Vgene, 5/6 = Lgene, 5/6 ωgene, 5/6 (22)
This velocity depends on the length of a gene
(Lgene, 5/6) and its rotating velocity (ωgene, 5/6). Lgene, 5/6 = 2×10-12 m (19, 20) (23)
The rotating velocity of a gene (ωgene, 5/6) can be obtained by summing over rotating velocities of all its effective charges (ωcharge, 5/6): ωgene, 5/6 = ncharge, 5/6 ωcharge, 5/6 (24) To obtain the number of charges, we multiply number of bases and number of atoms/electrons
ncharge, 5/6 = 2Nbase Natom (25)
Now, we put approximate values for numbers and obtain velocity of genes:
Substituting values of velocity from equation (32) and charges from equation (21) in equation (16), we can obtain the current of genes:
Igene, 5/6 ~ 10-3 (33)
Putting the current from the above equation (33) and density of genes from equation (15) in equations (6-10), we calculate magnetic fields of a DNA within a cell.
Substituting the above equation in equations (1- 3), we can obtain the probability for the amount of effects of external fields on the evolutions of DNAs within a cell:
PDNA = exp (KS EDNA / Tcell) / ΩDNA, tot (42)
Fig. 6. The probability of the effect of waves on the evolutions of a DNA within a cell in terms of wavelength The above probability depends on the wavelength of external fields.
In Fig. 6, we show the probability for producing hexagonal and pentagonal DNA holes within a cell. This figure indicates that by decreasing the wavelength (< 10⁻³m), waves pass the cell membrane and interact with DNAs. This interaction causes the motions of DNAs. By motions of DNAs, their charges move and emit strong waves. These waves produce hexagonal and pentagonal holes within a cell. To fill these holes, extra bases are produced. These bases could join to each other and form viruses such as COVID-19.
DISCUSSION
Our results show that, by decreasing the wave length, waves emitted from towers in 5G and higher technologies could have more effect on evolutions of DNAs within cells. This is because dermatologic cell membranes act as an antenna for these waves. They are built from charged particles,such as electrons and atoms, and could emit or receive waves. On the other hand, an antenna could only take waves in which their lengths are not greater than its size. Thus, a cell membrane could take millimeter waves in 5G technology. These waves could pass the membrane and interact with biological matters within a cell.
If wavelengths of 5G waves be equal or less than the size of a nucleus, they can pass the nuclear membrane and interact with DNAs. These DNAs are built from hexagonal and pentagonal bases and, by their motions, some holes emerge. These holes are filled by hexagonal and pentagonal extra bases which are constructed by cells. These bases could join to each other and form some viruses such as Coronavirus. It is concluded that in the next generation of mobile technology, emitted waves of towers will have more effects on biological cells.
In this research, we have shown that new generation mobile technology, like 5G, could have the main role in constructing various types of viruses, such as Coronaviruses, within a cell. Some wavelengths in these technologies are smaller than the size of biological cells and could pass the cell membrane and enter the nucleus. These waves could be taken by dermatologic antenna, transfer to host cells, interact with DNAs and move them. A DNA is formed from charged particles and, by its motions, electromagnetic waves emerge. These waves produce hexagonal and pentagonal holes in liquids within nucleus and the cell. To fill these holes, bases are produced. These bases join to each other and can construct viruses like Corona viruses.
REFERENCES
Baud D, Qi X, Nielsen-Saines K, Musso D, Pomar L, Favre G. Real estimates of mortality following COVID-19 infection. Lancet Infect Dis 2020; S1473-3099(20)30195-X.
Sexton NR, Smith EC, Blanc H, Vignuzzi M, Peersen OB, Denison MR. Homology-based identification of a mutation in the coronavirus rna-dependent rna polymerase that confers resistance to multiple mutagens. J Virol 2016; 90:7415-28.
Fehr AR, Perlman S. Coronaviruses: an overview of their replication and pathogenesis. Methods Mol Biol 2015; 1282:1-23.
Wang C, Horby PW, Hayden FG, Gao GF. A novel coronavirus outbreak of global health concern. Lancet 2020; 395:470-73.
Hui DS, I Azhar E, Madani TA, et al. The continuing 2019-nCoV epidemic threat of novel coronaviruses to global health – The latest 2019 novel coronavirus outbreak in Wuhan, China. Int J Infect Dis 2020
Arora G, Kassir M, Jafferany M, et al. The COVID-19 outbreak and rheumatologic skin diseases. Dermatol Ther 2020; e13357.
Betzalel N, Ishai PB, Feldman Y. Environmental Research 2018; Volume 163, p. 208-216.
Rappaport TS, Sun S, Mayzus R, et al. Millimeter wave mobile communications for 5G Cellular: it will work! IEEE Access 2013; 1:335-49.
Nordrum A, Clark K. Everything you need to know about 5G”. IEEE Spectrum magazine 2017.
Saracco R. Taking a fresh look at 5G – Technology enablers I. IEEE Future Directions 2019.
Kostoff RN, Heroux P, Michael A, Tsatsakis A. Adverse health effects of 5G mobile networking technology under real-life conditions. Toxicol Lett2020; 323:35-40.
Christianto V, Boyd RN, Smarandache F. Wireless Technologies (4G, 5G) are very harmful to human health and environment: a preliminary review. BAOJ Cancer Res Ther 2019; 5:25:066.
Miller WB Jr, Torday JS, Baluška F. The N-space Episenome unifies cellular information space-time within cognition-based evolution. Prog Biophys MolBiol 2020; 150:112-39.
Baluška F, Miller WB Jr. Senomic view of the cell: Senome versus Genome. Commun Integr Biol 2018; 11:1-9.
Rattemeyer M, Popp FA, Nagl W. Evidence of photon emission from DNA in living systems. Naturwissenschaften 1981; 68:572-73.
Sepehri A. A mathematical model for DNA. Int J Geom Methods Mod Phys 2017; 14: No. 11, 1750152.
Redon R, Ishikawa S, Fitch KR, et al. Global variation in copy number in the human genome. Nature 2006; 444:444-54 .
Allfrey VG, Mirsky AE. Structural modifications of histones and their possible role in the regulation of RNA synthesis. Science 1964; 144:559.
Dolezel J, Bartoš J, Voglmayr H, Greilhuber J. Nuclear DNA content and genome size of trout and human. Cytometry Part A 2003; 51:127-28.
Greilhuber J, Doležel J, Lysák M, Bennett MD. The origin, evolution and proposed stabilization of the terms ‘genome size’ and ‘C-value’ to describe nuclear DNA contents. Ann Bot 2005; 95:255-60.
Abecasis GR, Auton A, Brooks LD, et al. An integrated map of genetic variation from 1,092 human genomes. Nature 2012; 491(7422):56-65.
Auton A, Brooks LD, Durbin RM, et al. A global reference for human genetic variation. Nature 2015; 526:68-74.
Department of Clinical and Experimental Medicine, University of Foggia, Italy
2. Department of Experimental Medicine, Section of Human Physiology and Unit of Dietetics and Sports Medicine, Università degli Studi della Campania Naples, Italy
3. Department of History, Society and Studies on Humanity, University of Salento, Lecce Italy
4. Department of Law, Forensic Medicine, Magna Graecia University of Catanzaro, Italy
5. Department of General Surgery and Medical-Surgical Specialties, University of Catania, Italy
6. Department of Mental Health, Physical and Preventive Medicine, Clinic of Child and Adolescent Neuropsychiatry, Università degli Studi della Campania Italy
7. Department of Education Sciences, Psychology and Communication, University of Bari, Italy
Abstract
Background: On the 31 December 2019, the World Health Organization (WHO) was informed of a cluster of cases of pneumonia of unknown origin detected in Wuhan City, Hubei Province, China.
The infection spread first in China and then in the rest of the world, and on the 11th of March, the WHO declared that COVID-19 was a pandemic. Taking into consideration the mortality rate of COVID-19, about 5–7%, and the percentage of positive patients admitted to intensive care units being 9–11%, it should be mandatory to consider and take all necessary measures to contain the COVID-19 infection.
Moreover, given the recent evidence in different hospitals suggesting IL-6 and TNF-α inhibitor drugs as a possible therapy for COVID-19, we aimed to highlight that a dietary intervention could be useful to prevent the infection and/or to ameliorate the outcomes during therapy. Considering that the COVID-19 infection can generate a mild or highly acute respiratory syndrome with a consequent release of pro-inflammatory cytokines, including IL-6 and TNF-α, a dietary regimen modification in order to improve the levels of adiponectin could be very useful both to prevent the infection and to take care of patients, improving their outcomes.
1. Background
On the 31 December 2019, the World Health Organization (WHO) was informed of a cluster of cases of pneumonia of unknown origin detected in Wuhan City, Hubei Province, China. About one month later (on 8 January 2020), the Chinese authorities declared the identification of a new type of coronavirus, informing the WHO a few days later that the outbreak was associated with exposure in a seafood market in Wuhan City.
The infection spread firstly in China and then in the rest of the world, and on the 11th of March, the WHO declared that COVID-19 was a pandemic.Coronaviruses (CoVs) belong to the subfamily Orthocoronavirinae in the family of Coronaviridae in the order Nidovirales, and this subfamily includes α-coronavirus, β-coronavirus, γ-coronavirus, and delta-coronavirus [1].
Coronaviruses primarily cause enzootic infections in birds and mammals and, in the last few decades, have shown to be capable of infecting humans as well [2]. In human infections with highly virulent respiratory viruses—such as avian influenza H5N1, H7N9, Severe Acute Respiratory Syndrome (SARS) coronavirus, and Coronavirus Disease-19 (COVID-19)—immunopathogenesis caused by the overproduction of pro-inflammatory cytokines may play an essential role in disease progression and mortality [3].
Several recent studies have reported that COVID-19 caused the destruction of the pulmonary parenchyma, including interstitial inflammation and extensive consolidation, similarly to the previously reported coronavirus infection [4,5]. During coronavirus infection, it was observed that the lungs increased in weight, with a mild pleural effusion of clear serous fluid, named pulmonary edema, and extensive consolidation [6,7]. In some areas, there was interstitial thickening, with mild-to-moderate fibrosis, but a disproportionately sparse infiltrate of inflammatory cells (mainly histiocytes, including multinucleated forms, and lymphocytes) [8]. A dilatation of the airspaces was observed, as was focal honeycombing fibrosis. An intra-alveolar organization of exudates was described, and the formation of granulation tissues in the small airways and airspaces was reported. These lesions were typically located in the sub-pleural region, and the cellular component mainly consisted of histiocytes, as reported in a previous paper [9]. Xu et al. described in their case report the pathological findings of COVID-19 associated with acute respiratory distress syndrome. At the X-ray investigation, they detected a rapid progression of bilateral pneumonia.
The biopsy samples were taken from the lung; the histological examination showed bilateral diffuse alveolar damage with cellular fibromyxoid exudates [6].Considering that the mortality rate of COVID-19, about 5–7% [10], and the percentage of positive patients admitted to intensive care units being 9–11% [11], it should be mandatory to consider and take all necessary measures intended to contain the viral infection.
A recent study analyzed the data of 150 COVID-19 patients, with the aim of defining the clinical predictors of mortality. The results obtained from this study suggest that COVID-19 mortality might be due to virus-activated “cytokine storm syndrome”, considering that the plasma levels of IL-6 were higher in deceased patients compared to in discharged subjects [12].Considering that a detailed study has not been performed on the immunological response to COVID-19, the only way to discuss this thematic is to refer to previous knowledge about SARS-CoV and MERS-CoV. The first response is obtained through pattern recognition receptors (PRRs) including C-type lectin-like receptors, Toll-like receptors (TLR), NOD-like receptors (NLR), and RIG-I-like receptors (RLR). Moreover, several inflammatory factors are expressed such as IL-6 and TNF-α; moreover, the synthesis of type I interferons (IFNs) is activated, and these exert their actions against virus diffusion, accelerating macrophage phagocytosis [13] (Figure 1).
Figure 1. The main immunological response to COVID-19.
In the light of these considerations and the recent evidence in different hospitals suggesting IL-6 and TNF-α inhibitor drugs as a possible therapy for COVID-19, this review aims to highlight how a dietary intervention could be useful to prevent the infection and/or to ameliorate the outcome during therapy.
2. The Pivotal Role of IL-6 and TNF-α in Lung Infections
The first laboratory report about COVID-19 patients indicated several parameters that were found to be altered in blood samples; for example, D-dimer, neutrophil count, blood urea, and creatinine levels were significantly higher. In the same way, several cytokines such as IL-6 and TNF-α were overexpressed, indicating the immune status of the patients [14].IL-6 represents pro-inflammatory signaling produced by adipose tissue; for this reason, this endocrine cytokine could be important in regulating the host response during acute infection [15].
Several papers have described the essential role of IL-6 in generating a proper immune response during different kinds of viral infection in the pulmonary tract. Others link this cytokine to an exacerbation of viral disease. These latter findings support the hypothesis that IL-6 upregulation during viral infections may promote virus survival and the exacerbation of the clinical disease [16,17].
Indeed, IL-6 has a pleiotropic function, and it is produced in response to tissue damage and infection. In particular, at the pulmonary level, innate and adaptative immune cell proliferation is strongly influenced by this cytokine. After targeting its specific receptor, IL-6 starts a cascade of signaling events mainly associated with the JAK/STAT3 activation pathway, promoting the transcription of multiple downstream genes related to cellular signaling processes, including cytokines, receptors, adaptor proteins, and protein kinase [15].
Furthermore, it has been reported that IL-6 is an essential factor for the survival of mice with a viral infection. This cytokine promotes the optimal regulation of the T-cell response, inflammatory resolution, tissue remodeling promoting lung repair, cell migration, and the phagocytic activities of macrophages, as well as preventing virus-induced apoptosis in lung epithelial cells.
However, experimental scientific evidence also suggests potential adverse consequences that increased levels of IL-6 might have on the cellular immune response against viruses. In this context, different possible mechanisms involving this cytokine might affect viral clearance, ultimately favoring the establishment of a persistent viral state in infected hosts [18,19].
Tumor necrosis factor is a cell-signaling protein (cytokine) involved in systemic inflammation, released predominately from macrophages, but it is also released from a variety of other immune cells. It has been well described that during infection with the influenza virus, the expression of TNF-α in lung epithelial cells was higher, exerting powerful anti-influenza virus activity [20].
In an animal model, it has been demonstrated that TNF-α plays a pivotal role in the development of pulmonary fibrosis. TNF-α signals via two receptors, TNF-RI and TNF-RII; the first receptor (TNF-RI) promotes intracellular signaling involving c-Jun N-terminal kinase (JNK) and nuclear factor (NF)-κB, while the other receptor, TNF-RII, promotes TNF-RI–dependent cell death, without directly inducing apoptosis. Although both receptors are broadly expressed, it is known that the majority of inflammatory signaling is elicited through TNF-RI [21].
In an in vitro model, it has been described that serine/threonine kinases can phosphorylate TNF-RI and its molecules, preventing tyrosine phosphorylation [22,23,24].In patients with COVID-19, the high serum levels of IL-6 and TNF-α are negatively correlated to T cells; contrariwise, it has been demonstrated that T cell levels were restored by reducing IL-6 and TNF-α concentrations [25]. These findings suggested that these cytokines could represent important targets of anti-COVID-19 therapies.
3. Adiponectin Function in Lung Infections
Through the secretion of adipokines, adipose tissue participates in the regulation of several pathophysiological processes in many organs and tissues. Among the adipokines, adiponectin is the most relevant. Adiponectin is one of the most abundant circulating adipocytokines, accounting for 0.01% of total serum protein. Adiponectin is an important regulator of cytokine responses, and this effect is isoform-specific. It is involved in a wide variety of physiological processes, including energy metabolism, inflammation, and vascular physiology. These effects are mediated by two atypical, widely expressed seven-transmembrane receptors, AdipoR1 and AdipoR2 [26]. Adiponectin has beneficial effects in cardiovascular systems and blood vessels, protecting these tissues through the inhibition of pro-inflammatory and hypertrophic responses and stimulation of endothelial cell responses [27].
Adiponectin circulates as three different isoforms (low molecular weight—LMW, medium molecular weight—MMW, and high molecular weight—HMW) [28].Infectious diseases are characterized by an increased production of adiponectin. Several papers suggest that adiponectin may be related to disease activity and/or severity in different conditions such as rheumatoid arthritis, osteoarthritis, and systemic lupus erythematosus. Since adiponectin has been found to display both pro- and anti-inflammatory activities, controversial findings have been observed regarding the role of total adiponectin in systemic autoimmune and inflammatory joint diseases. For this reason, the relative contribution of each adiponectin isoform to the inflammatory response and joint and/or tissue damage requires further study [29].
It is reported that adiponectin is regulated by transcription factors in adipose tissue, such as peroxisome proliferator-activated receptor-γ (PPAR-γ) [30]. During viral infections, it has been reported that the role of the predisposition of hosts is also important, as well as their state of health and nutrition. Indeed, it is well known that white adipose tissue is considered an endocrine source of biologically active substances with local and/or systemic action, called adipokines.
The inappropriate secretion of adipokines seems to participate in the pathogenesis of obesity-related diseases, including endothelial dysfunction, inflammation, and atherosclerosis [31,32,33].The biological function of adipokines in lung diseases seems to be mainly related to the inflammatory process. In particular, the intercorrelation between adipose tissue and the lung has become evident as the involvement of adiponectin has been demonstrated in several lung diseases such as Chronic Obstructive Pulmonary Disease (COPD), emphysema, and cancer [34]. In fact, with specific regard to COPD, a low-grade inflammatory state has been demonstrated [35,36,37].
Moreover, increasing evidence suggests that adiponectin also exerts a crucial role in the vascular endothelium, maintaining vascular homeostasis and protecting against vascular dysfunctions. Altogether, these findings support the anti-inflammatory role of adiponectin in COPD and, in general, in other lung diseases [38].The critical role of adiponectin in the pathophysiological conditions of the lung is also supported by the modulation of AdipoRs with the downregulation of AdipoR2. It has been described that the adiponectin oligomerization state is altered in COPD; moreover, the presence of AdipoR1 and AdipoR2, with a lower expression of AdipoR2 compared to AdipoR1, in lung tissue [39] has been demonstrated. The low expression of AdipoR2 could suggest a specific role of this receptor, mainly implicated in adiponectin’s effects on inflammation and oxidative stress. Mainly, it has been observed that higher levels of adiponectin are associated with a significant and specific increase in HMW adiponectin, representing the most biologically active forms. Thus, HMW adiponectin increases IL-6 secretion in human monocytes and human monocytic leukemia cell lines but does not suppress lipopolysaccharide (LPS)-induced IL-6 secretion. Byn contrast, LMW adiponectin reduces LPS-mediated IL-6 release and also stimulates IL-10 secretion [40].
Furthermore, several in vitro studies have demonstrated that adiponectin in the A549 adenocarcinoma human alveolar basal epithelial cell line has an essential apoptotic effect and also reduces the production of pro-inflammatory cytokines such as TNF-α, blocking NF-κB nuclear translocation [41,42].Indeed, adiponectin can reduce innate and adaptive immune cell proliferation and polarization, also blocking the production of pro-inflammatory cytokines such as TNF-α, IL-2, and IL-6, and enhancing that of anti-inflammatory cytokines such as IL-10, with a decrease in the phosphorylation of AMPK, p38, ERK1/2, and c-JNK [43,44,45,46]. Data from in vitro studies on lung cells were consistent with an anti-inflammatory function of adiponectin, and adiponectin-deficient mouse models developed lung function impairments and systemic inflammation [47].
The possible role of adiponectin in inflammatory pulmonary diseases, such as asthma and chronic obstructive pulmonary disease (COPD), and in critical illnesses has been the subject of recent investigations. Particularly, the HMW isoform has a specific role in pulmonary diseases and critical illnesses, even if its role should be better clarified [48,49].
An interesting study reported that systemic adiponectin concentrations in humans fall during the acute phase of lung infection: particularly, during the early phase, the pro-inflammatory state is generated by the high systemic TNF-α and IL-6 concentrations, with the subsequent inhibition of adiponectin production. Contrariwise, it has been described that the reduction in TNF-α and IL-6 factors generates a corresponding bounce-back in systemic adiponectin concentrations [50].
Although it is still unclear whether the modulation of systemic adiponectin or its signaling pathways has any therapeutic benefit in pulmonary or critical illnesses, it may serve as a novel therapeutic or preventative tool for these illnesses in the future. One obvious pharmaceutical treatment would be the exogenous administration of adiponectin by the inhalational or intravenous route. Although this has been tried in mouse models [51], the problems to be overcome prior to human administration include establishing what the biologically active molecule is and what role post-translational modifications have upon its function, and the associated difficulties in generating biologically active molecules on a large scale.
Considering the difficulty linked to the direct administration of adiponectin, in the last few years, other drugs have been used that indirectly improve adiponectin production. For example, a synthetic ligand of peroxisome proliferator-activated receptors can increase adiponectin mRNA in adipocytes, improving the production and secretion of adiponectin [52,53,54,55]. Moreover, other drugs such as fibrates can increase systemic adiponectin levels by enhancing PPAR-γ activity [56,57]. Another way to improve adiponectin levels is the use of angiotensin converting enzyme inhibitors [58,59,60]. Furthermore, it is possible to stimulate adipocyte differentiation [61] and the activation of PPAR [62].
Finally, it has been described that calcium channel blockers [63] and a central-acting anti-hypertensive agent [64] also increase systemic adiponectin concentrations [65]. The possibility to improve the action of adiponectin through diet is intriguing; it has been described that nutritional interventions may help to regulate systemic adiponectin concentrations. In an animal model, it has been demonstrated that a diet with a high concentration of polyunsaturated fatty acids and supplemented with ω-3 can improve the plasma levels of adiponectin, increasing gene expression [66]. On the other hand, in humans, adiponectin levels are positively associated with a healthy lifestyle and the Mediterranean diet, even if the mechanisms of action are not completely known [66]. Finally, in light of these considerations, in COVID-19 therapy, it could be very useful to combine drug therapy with a specific diet regimen.
4. ω-3 PUFAs and Lung Infections
Another important mediator involved in the immune response and influenced by nutrition are fatty acids, in particular, ω-3 PUFAs [67,68]. In fact, during bacterial and viral infections, they are able to act on immune cells and regulate diverse inflammatory processes. ω-3 PUFAs are known to have anti-inflammatory properties and play an essential role in the resolution of inflammation [69].
In several lung infections, the administration of PUFA can ameliorate the outcome of the patient in acute pneumonia. Sharma et al. reported in their study that the dietary supplementation of ω-3 PUFA can exert an overall beneficial effect against acute pneumonia through the upregulation of the host’s specific and nonspecific immune defenses [70]. ω-3 polyunsaturated fatty acids (PUFA, ω-3-fatty acids), the key components of fish and flaxseed oils, are increasingly consumed by the public because of their potential health benefits and can be used clinically for the treatment of metabolic, cardiac, inflammatory, and autoimmune diseases [71].
However, numerous studies have shown that these compounds are immunoregulatory and immunosuppressive and thus may increase susceptibility to infection. While reports suggest that ω-3 PUFAs may have beneficial effects against extracellular pathogens, few studies have been performed on systemic viral infections in mammals. Jones and Roper described in their study that a diet rich in ω-3 PUFAs did not significantly lower survival of the vaccinia virus infection, at least with short-term (~6 week) feeding in mice [71].
ω-3 PUFAs are metabolized into various mediators possessing anti-inflammatory properties such as resolvins and protectins. It is known that ω-3 PUFAs can reduce NF-κB activation by preventing nuclear p65 NF-κB translocation. Furthermore, ω-3 PUFAs minimize the activation of ERK1/2 MAPK, also reducing COX-2 production. The ω-3 PUFA-derived lipid mediator could markedly attenuate influenza virus replication via the RNA export machinery. In addition, the treatment of protectin D1 with peramivir could completely stop mouse mortality [72].
ω-3 supplementation was previously studied in Acute Respiratory Distress Syndrome (ARDS). Singer and Shapiro suggested that the enteral administration of natural antioxidant substances could improve oxygenation and clinical outcomes in ICU patients [73]. A systematic review performed in 2015 reported a positive effect only for patients suffering from ARDS with high mortality [74]. A more recent meta-analysis highlighted the importance of clinical trials in order to clarify the use of ω-3 fatty acids and antioxidants in patients with ARDS to ascertain the positive effects in order to reduce the lengths of ICU stays and the numbers of days spent on ventilators [75].
Although the role of ω-3 supplementation in ARDS should be better clarified, its pivotal role in reducing reactive oxygen species and pro-inflammatory cytokines, such as TNF-α, IL-1β, IL-6, and IL-8 [76], is well known.Therefore, ω-3 PUFAs, including protectin D1, which is a novel antiviral drug, could be considered for potential interventions for COVID-19.
5. Other Dietary Constituents and Lung Infections
As previously described, other dietary constituents can be used to improve the patients’ outcomes during lung infection, regulating the inflammatory response. Among these, antioxidants play an important role in protecting lung cells against viruses and bacteria. Viral infection leads to an increase in the intrapulmonary oxidative burden. In many diseases, the balance between oxidants and antioxidants (redox balance) is altered, with severe consequences [77].
The pathophysiological mechanisms by which free radicals generate various types of stress—such as oxidative, nitrative, carbonyl, inflammatory, and endoplasmic reticulum stress—lead to lung inflammation and an altered lung immune response. In this scenario, dietary antioxidants may play an important role against lung oxidative stress [77].
Several studies reported the protective role of the antioxidants in lung infection and in lung inflammation [78,79].In particular, vitamin C, polyphenols, and flavonoids can play a protective role in lung infections, being immune modulators and inflammatory mediators. Indeed, as reported by Carr et al., during infection, vitamin C levels may become depleted; for this reason, vitamin C supplementation can attenuate infection. Based on this evidence, these authors suggested a clinical trial with vitamin C infusion for the treatment of severe COVID-19 patients [80].
Among polyphenols, epigallo-catechin 3 gallate (EGCG) is the most potent ingredient in green tea and exhibits antibacterial, antiviral, antioxidative, anticancer, and chemo-preventive activities. Recently, numerous studies have investigated the protective effects of EGCG against asthma and other lung diseases such as COPD and lung pneumonia. EGCG may suppress inflammation and inflammatory cell infiltration into the lungs of asthmatic mice, and may also inhibit epithelial-mesenchymal transition EMT via the PI3K/Akt signaling pathway through upregulating the expression of phosphatase and tensin homolog (PTEN), both in vivo and in vitro [81].
Moreover, flavonoids can be used to attenuate lung injury in mice; it has been reported that they inhibit influenza virus and Toll-like receptor signaling, blocking NF-κB translocation [82].Therefore, as summarized in Table 1, supplementation with vitamin C, flavonoids, and polyphenols can be tested in COVID-19 patients, both in order to prevent viral infection and to improve patients’ outcomes.
Table 1. The principal antioxidants involved in lung infection and the immune-inflammatory response.
6. Discussion and Conclusions
During pulmonary infections, and particularly in COVID-19 patients, intracellular signaling leads to the production of pro-inflammatory cytokines, such as TNF-α and IL-6, which act in concert with chemoattractants, such as CXCL1 and CXCL2, to recruit polymorphonuclear leukocytes (PMNs) to the lungs, killing pathogens but generating fibrosis [83].
Another important consideration during COVID-19 infection is related to the modification of the secretory products of the upper and lower airways, which usually include mucin and pulmonary surfactant. During infection, mucin production is upregulated, with the function of preventing microbes from binding to and infecting epithelial cells [84].
The primary source of phospholipids (PLs) in the lung is pulmonary surfactant, synthesized and released by alveolar epithelial type II cells. The surfactant contains approximately 80–90% PLs, with fatty acid chains that can be oxidized during different challenges in the lung [85]. The oxidation of these PLs in the lung can occur in the setting of an increased oxidative stress situation, such as infection and inflammation [86]. The immune effects of oxidized phospholipids oxPLs during infectious diseases are inevitably dictated by the balance among activation, degradation, and scavenging. It has been shown that oxPLs are generated in the lung during several pulmonary infections, including influenza and avian influenza (H5N1), as well as SARS coronavirus, even if the mechanisms of action are not well known [87,88,89].
As reported by Imai et al., oxPL-induced inflammation is mediated by TLR4 and TRIF, driving an increase in IL-6 production [89]. It is intriguing to consider that oxPL-dependent defects in phagocytosis and ROS generation may lead to an increased susceptibility to respiratory infections [90]. Cholesterol is the major neutral lipid in pulmonary surfactant, in which it is thought to promote the spreading, mobility, and adsorption of surfactant films [91].
As previously documented, modulating adiponectin levels can be considered an important way to reduce cytokines levels; in this way, the adverse effects related to the COVID-19 infection should be attenuated. It is well described in animal models that the consumption of hyperlipidemic diets, rich in saturated fat, reduces the levels of adiponectin, while diets rich in polyunsaturated fatty acids and supplemented with ω-3 PUFA increase adiponectin levels, reducing pro-inflammatory cytokines [66].Innate and adaptive immune responses are influenced not only by oxPLs and cholesterol but also by the fatty acid profiles of tissues in response to pharmacological agents and diet [92].
Several studies performed in animal models demonstrated how ω-3 PUFA uptake into the lung tissue influences outcomes associated with infection, promoting the resolution of inflammation [93]. In another study, ω-3 PUFAs reduced the levels of PMNs and lowered IL-6 levels in lung infections [94]. These positive effects remain controversial; for example, Jones and Roper reported that in their experimental model, no statistically significant differences were found among the diet regimens, with and without ω-3 PUFAs, with respect to the susceptibility of mice to viral infection, morbidity, viral organ titers, recovery time, or mortality [71].
In conclusion, it is well known that general treatments are very important to enhance the host immune response against RNA viral infection. In addition, the immune response has often been shown to be weakened by inadequate nutrition in many model systems as well as in human studies. However, the nutritional status of the host, until recently, has not been considered as a contributing factor to the emergence of viral infectious diseases. The recent reports about the pathogenesis of COVID-19 suggested that one of the most important consequences of this infection is the cytokine storm syndrome [95], which could be strictly linked with coagulopathy, generating acute pulmonary embolism caused by in-situ thrombosis [96,97]. Therefore, a great number of clinical trials are ongoing to define a useful therapy to attenuate cytokine storms [98].For these reasons, an adequate ω-3 PUFA intake may be a valid strategy against viral infection.
Indeed, following the recommended intake of ω-3 PUFA, in the range of 0.5% and 2% of total calories (250 mg/day), may be important to protect against an excessive inflammatory response, also reducing IL-6 levels. This theory found important support in a recent study that demonstrated that ω-3 PUFA-derived lipid mediator protectins can suppress influenza virus replication through a mechanism that blocks the export of viral mRNA. Moreover, Imai demonstrated that this mediator can be used in combination with the antiviral peramivir, even at late time points in infection [99].
Nevertheless, the efficacy of ω-3 PUFAs at the clinical level is under investigation; for example, Hecker et al. described a beneficial effect for a diet regimen with ω-3 PUFAs, describing that the pro-inflammatory cytokine levels decreased after this diet regimen [100]. The suggested positive role in the outcome and prevention of the COVID-19 infection is summarized in Figure 2.
Figure 2. Adiponectin and ω-3 PUFAs reduce the lung inflammation that occurs following coronavirus infection, reducing IL-6 production, ERK1/2, and COX-2 activation and the nuclear translocation of NF-κB.
In addition, adiponectin plays a role in lung diseases and obesity; in the development and progression of lung disease and cancer, a pathogenic role of adiponectin was defined by both in vivo and in vitro studies.
Recently, immunometabolic pathomechanisms have been identified as important factors determining and modulating lung function and disease. Particularly, adiponectin levels have been found to be greater in patients with COPD compared with in control patients, and adiponectin-deficient mice are protected from several lung diseases [101].
Moreover, it has been reported that adherence to the Mediterranean diet was associated with an increase in adiponectin levels, improving cardiovascular system functionality [102], particularly in elderly people [103]. These findings are only apparently contradictory to the first data about the mortality rate from COVID-19 infections in the Mediterranean area (such as in Italy and Spain) [104].
First of all, the data have been referred only to the tested population; moreover, it is well described that the presence of several comorbidities such as hypertension, diabetes, and cardiovascular diseases severely influenced the mortality rate reported in this area [105].
All these comorbidities can be counteracted with a correct dietary regimen. Therefore, both adiponectin and ω-3 PUFAs appear to be attractive biomarkers for monitoring lung disease progression.
Finally, considering that the COVID-19 infection can generate a mild or highly acute respiratory syndrome with a consequent release of pro-inflammatory cytokines, including IL-6 and TNF-α, a modification of the dietary regimen in order to improve the levels of adiponectin could be very useful both to prevent the infection and to take care of the patients, improving their outcomes.
Given the similar pathway of action, it can be hypothesized that adiponectin and ω-3-PUFA could be used as real drugs to reduce inflammation, reducing both IL-6 and TNF-α levels as well as ameliorating the lung damage that occurs following coronavirus infection.