Anxiety disorders, such as phobias and posttraumatic stress disorder, are among the most common mental disorders.
Cognitive therapy helps in treating these disorders; however, many cases relapse or resist the therapy, which justifies the search for cognitive enhancers that might augment the efficacy of cognitive therapy.
Studies suggest that enhancement of plasticity in certain brain regions such as the prefrontal cortex (PFC) and/or hippocampus might enhance the efficacy of cognitive therapy. We found that elevation of brain magnesium, by a novel magnesium compound [magnesium-l-threonate (MgT)], enhances synaptic plasticity in the hippocampus and learning and memory in rats. Here, we show that MgT treatment enhances retention of the extinction of fear memory, without enhancing, impairing, or erasing the original fear memory.
We then explored the molecular basis of the effects of MgT treatment on fear memory and extinction. In intact animals, elevation of brain magnesium increased NMDA receptors (NMDARs) signaling, BDNF expression, density of presynaptic puncta, and synaptic plasticity in the PFC but, interestingly, not in the basolateral amygdala.
In vitro, elevation of extracellular magnesium concentration increased synaptic NMDAR current and plasticity in the infralimbic PFC, but not in the lateral amygdala, suggesting a difference in their sensitivity to elevation of brain magnesium.
The current study suggests that elevation of brain magnesium might be a novel approach for enhancing synaptic plasticity in a regional-specific manner leading to enhancing the efficacy of extinction without enhancing or impairing fear memory formation.
The serum levels of parathyroid hormone and magnesium depend on each other in a complex manner. The secretion of parathyroid hormone by the parathyroid is physiologically controlled by the serum calcium level, but magnesium can exert similar effects.
While low levels of magnesium stimulate parathyroid hormone secretion, very low serum concentrations induce a paradoxical block. This block leads to clinically relevant hypocalcemia in severely hypomagnesiemic patients.
The mechanism of this effect has recently been traced to an activation of the alpha-subunits of heterotrimeric G-proteins. This activation mimicks activation of the calcium sensing receptor and thus causes inhibition of parathyroid hormone secretion.
In addition to the effects of magnesium on parathyroid hormone secretion, parathyroid hormone in turn regulates magnesium homeostasis by modulating renal magnesium reabsorption. The distal convoluted tubule is of crucial importance for parathyroid hormone-regulated magnesium homeostasis.
Magnesium is a cofactor of different enzymatic reactions involved in anabolic and catabolic processes that affect muscular performance during exercise. In addition, it has been suggested that magnesium could participate in maintaining muscle integrity during demanding effort.
The main purpose of this study was to analyze the effects of magnesium supplementation in preventing muscle damage in professional cyclists taking part in a 21-day cycling stage race. Eighteen male professional cyclists (n = 18) from two teams were recruited to participate in the research.
They were divided into 2 groups: the control group (n = 9) and the magnesium-supplemented group (n = 9). The supplementation consisted of an intake of 400 mg/day of magnesium during the 3 weeks of competition.
Blood samples were collected according to World Anti-Doping Agency rules at three specific moments during competition: immediately before the race; mid competition; and before the last stage. Levels of serum and erythrocyte magnesium, lactate dehydrogenase, creatinine kinase, aspartate transaminase, alanine transaminase, myoglobin, aldolase, total proteins, cortisol and creatinine were determined.
Serum and erythrocyte magnesium levels decreased during the race. Circulating tissue markers increased at the end of the race in both groups. However, myoglobin increase was mitigated in the supplemented group compared with the controls. We conclude that magnesium supplementation seems to exert a protective effect on muscle damage.
Background: Physical exercise activates the hypothalamo-pituitary-adrenal (HPA) axis and induces the body’s inflammatory response. Due to contemporary dietary habits and increased energy expenditure, athletes are susceptible to depletion of magnesium ions. The aim of our study was to investigate, through assessment of plasma ACTH, serum IL-6, and salivary/serum cortisol levels, if chronic magnesium supplementation might reduce damaging stress effects in amateur rugby players.
Methods: Rugby players (N=23) were randomly assigned to intervention and control group. Basal samples were collected before intervention group started a 4-week-long supplementation with magnesium (500 mg Mg/d). Blood and saliva sampling were done a day before the match (Day-1), on the morning of competition (Game), and during a six-day-long recovery period (Day1, Day3 and Day6). ACTH, serum/salivary cortisol, IL-6 and total/differential leukocytes counts were determined at each time point.
Results: There was a statistically significant increase in ACTH concentration in intervention group compared to control group, while reductions in cortisol concentrations between the two groups were the greatest at Day-1 (p < 0.01) and at the day of competition (Game) (p < 0.01). Our results revealed that magnesium completely abolished the increase in IL-6 level noted in control group on Day1 and Day3 vs. Day-1 (p < 0.01) and also diminished the rise in neutrophil/lymphocyte ratio in intervention group vs. control group (p < 0.01).
Conclusions: These results suggest the possibly important influence magnesium supplementation might have on the change of parameters of HPA axis activity and reduction of immune response activation following strenuous physical exercise such as a rugby game.
Sixty percent of cases of clinical depression are considered to be treatment-resistant depression (TRD). Magnesium-deficiency causes N-methyl-d-aspartate (NMDA) coupled calcium channels to be biased towards opening, causing neuronal injury and neurological dysfunction, which may appear to humans as major depression.
Oral administration of magnesium to animals led to anti-depressant-like effects that were comparable to those of strong anti-depressant drugs. Cerebral spinal fluid (CSF) magnesium has been found low in treatment-resistant suicidal depression and in patients that have attempted suicide. Brain magnesium has been found low in TRD using phosphorous nuclear magnetic resonance spectroscopy, an accurate means for measuring brain magnesium.
Blood and CSF magnesium do not appear well correlated with major depression. Although the first report of magnesium treatment for agitated depression was published in 1921 showing success in 220 out of 250 cases, and there are modern case reports showing rapid terminating of TRD, only a few modern clinical trials were found.
A 2008 randomized clinical trial showed that magnesium was as effective as the tricyclic anti-depressant imipramine in treating depression in diabetics and without any of the side effects of imipramine.
Intravenous and oral magnesium in specific protocols have been reported to rapidly terminate TRD safely and without side effects.
Magnesium has been largely removed from processed foods, potentially harming the brain.
Calcium, glutamate and aspartate are common food additives that may worsen affective disorders.
We hypothesize that – when taken together – there is more than sufficient evidence to implicate inadequate dietary magnesium as the main cause of TRD, and that physicians should prescribe magnesium for TRD. Since inadequate brain magnesium appears to reduce serotonin levels, and since anti-depressants have been shown to have the action of raising brain magnesium, we further hypothesize that magnesium treatment will be found beneficial for nearly all depressives, not only TRD.
Through my life I have often pondered, why do some people seem unable to resist the lure of addictive substances, and, why do certain individuals succumb to addiction?
It always seemed that there must be more to it than, “that so-and-so is a bad apple”, which seems to often be the unthinking response of those who suffer at the hands of friends or family members addictive behaviours.
So why is it? Why do some young adults fall into one addiction, then another, often replacing drugs with adrenaline addictions, or sports, or eating?
It is often noted that certain people have an “addictive personality”, what does that mean though? Might it be deep seated nutritional deficiencies, which make the “personality” addictive?
Addiction is a dysregulation of brain reward systems that progressively increases, resulting in compulsive drug use and loss of control over drug-taking.
Addiction is a brain disease.
There is evidence that magnesium deficit is involved in addiction to various addictive substances (heroin, morphine, cocaine, nicotine, alcohol, caffeine, and others). Magnesium is involved in all the stages of addiction. Magnesium deficit enhances the vulnerability to psychoactive substance addiction. Stress and trauma reduce the brain magnesium level and at the same time favor addiction development.
In experimental studies, administration of magnesium while inducing morphine dependence in rats reduced the dependence intensity. Magnesium reduces the NMDA receptor activity and the glutamatergic activity. Because stress and trauma induce hypomagnesemia with increased vulnerability to addiction, magnesium intake by people who are under prolonged stress could be a way to reduce this vulnerability and the development of addiction to different psychoactive substances.
Anxiety and depression appear to be associated with increases in drug-related harm and addictive substance use. Magnesium anxiolytic effect could be important for the antiaddictive action. Addiction is characterized by relapses. Magnesium deficiency may be a contributing factor to these relapses.
ChooseLife : As we can see clearly above, scientific studies show that Magnesuim deficiency has a crucial, central role in the etymology of addiction. So, if we unravel the web of fibres which form our actions, we can easily see that it is those who through their lives eat less foods bearing Magnesium, who are always going to become more susceptible to the slavery and bondage of addictions in their lives.
How can we blame the addict, when their body aches and yearns, for something to take away the unconscious strain that lack of Magnesium induces in the host?
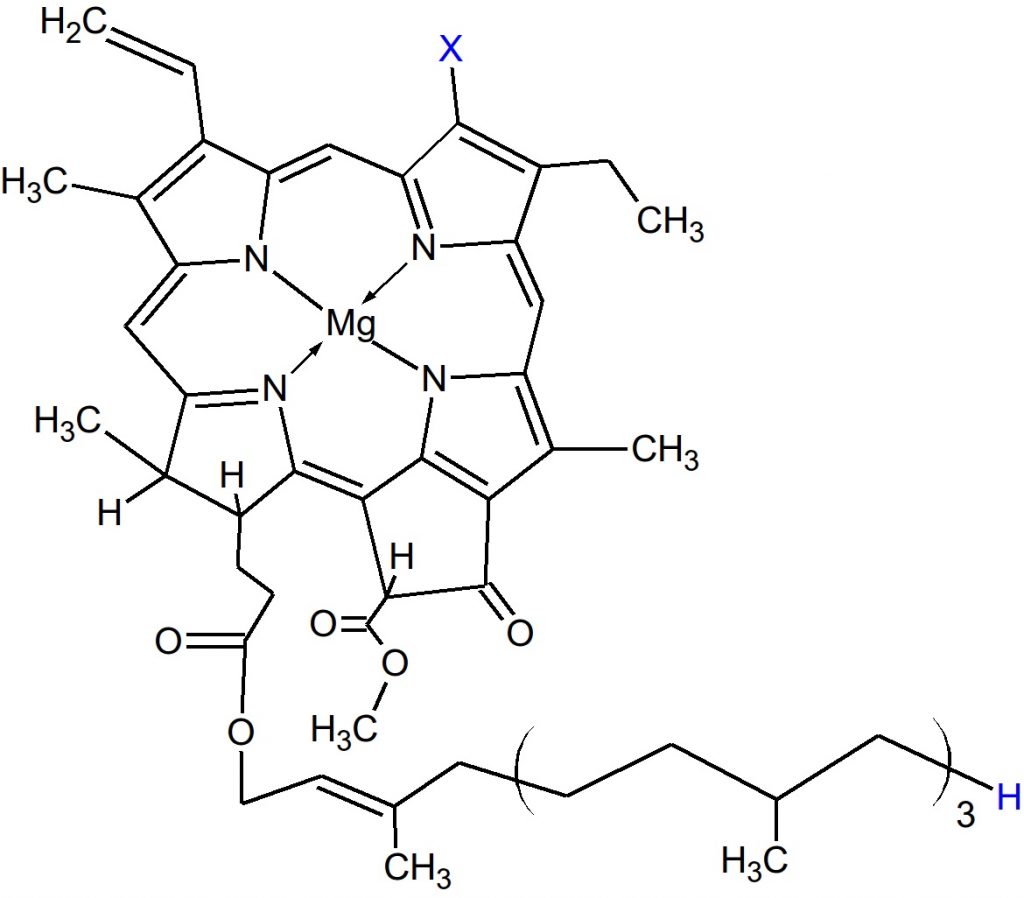
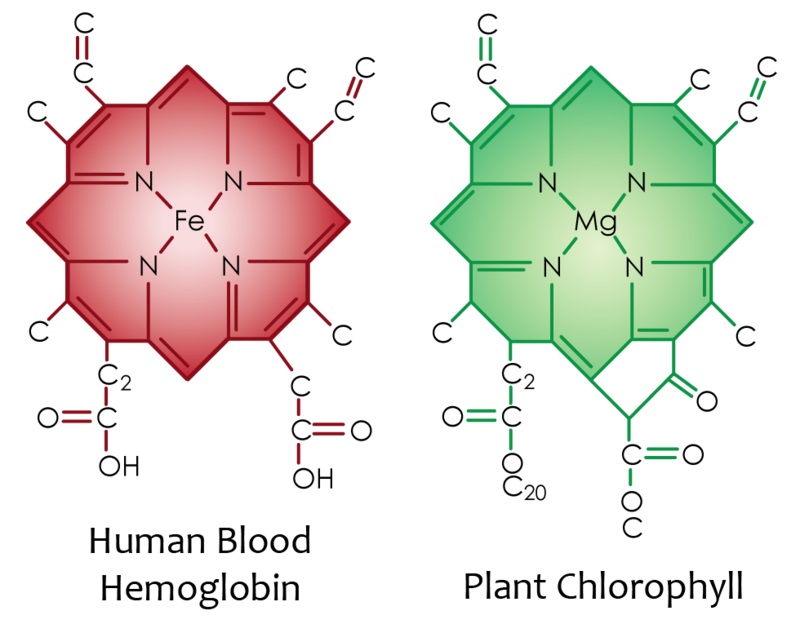
To be raised on a diet lacking in Greens, which have plentiful chlorophyll, which has Magnesium at its core:
How can it possibly be a childs fault? that he/she were not nurtured to eat a plentiful supply of this vital mineral? Or these health supporting foods?
This is not to blame the parents, where is the support from mental health services? Where are the warning campaigns that excessive simple sugars, or deficiencies in Magnesium and Omega3, are heavily implicated in numerous mental health conditions?
Are addicts, very often, simply self medicating?
It’s time to stop blaming the blood trickling from societies wounds.
ChooseLife : Here will begin a cursory search into the scientific literature, regarding Magnesium. From the start I should note, that Reams said Chlorophyll was vital to the Liver, that for the Liver to supply the Pancreas with sufficient enzymes for it to regulate sugars properly, we need equivalent to 3oz of green juice daily (probably more nowadays), at the centre of Chlorophyll? Magnesium:
Magnesium is well known for its diverse actions within the human body. From a neurological standpoint, magnesium plays an essential role in nerve transmission and neuromuscular conduction.
It also functions in a protective role against excessive excitation that can lead to neuronal cell death (excitotoxicity), and has been implicated in multiple neurological disorders.
Due to these important functions within the nervous system, magnesium is a mineral of intense interest for the potential prevention and treatment of neurological disorders.
Current literature is reviewed for migraine, chronic pain, epilepsy, Alzheimer’s, Parkinson’s, and stroke, as well as the commonly comorbid conditions of anxiety and depression.
Previous reviews and meta-analyses are used to set the scene for magnesium research across neurological conditions, while current research is reviewed in greater detail to update the literature and demonstrate the progress (or lack thereof) in the field. There is strong data to suggest a role for magnesium in migraine and depression, and emerging data to suggest a protective effect of magnesium for chronic pain, anxiety, and stroke.More research is needed on magnesium as an adjunct treatment in epilepsy, and to further clarify its role in Alzheimer’s and Parkinson’s. Overall, the mechanistic attributes of magnesium in neurological diseases connote the macromineral as a potential target for neurological disease prevention and treatment.
Major depression is a mood disorder characterized by a sense of inadequacy, despondency, decreased activity, pessimism, anhedonia and sadness where these symptoms severely disrupt and adversely affect the person’s life, sometimes to such an extent that suicide is attempted or results.
Antidepressant drugs are not always effective and some have been accused of causing an increased number of suicides particularly in young people.
Magnesium deficiency is well known to produce neuropathologies. Only 16% of the magnesium found in whole wheat remains in refined flour, and magnesium has been removed from most drinking water supplies, setting a stage for human magnesium deficiency.
Magnesium ions regulate calcium ion flow in neuronal calcium channels, helping to regulate neuronal nitric oxide production. In magnesium deficiency, neuronal requirements for magnesium may not be met, causing neuronal damage which could manifest as depression.
Magnesium treatment is hypothesized to be effective in treating major depression resulting from intraneuronal magnesium deficits. These magnesium ion neuronal deficits may be induced by stress hormones, excessive dietary calcium as well as dietary deficiencies of magnesium.
Case histories are presented showing rapid recovery (less than 7 days) from major depression using 125-300 mg of magnesium (as glycinate and taurinate) with each meal and at bedtime.Magnesium was found usually effective for treatment of depression in general use. Related and accompanying mental illnesses in these case histories including traumatic brain injury, headache, suicidal ideation, anxiety, irritability, insomnia, postpartum depression, cocaine, alcohol and tobacco abuse, hypersensitivity to calcium, short-term memory loss and IQ loss were also benefited. Dietary deficiencies of magnesium, coupled with excess calcium and stress may cause many cases of other related symptoms including agitation, anxiety, irritability, confusion, asthenia, sleeplessness, headache, delirium, hallucinations and hyperexcitability, with each of these having been previously documented. The possibility that magnesium deficiency is the cause of most major depression and related mental health problems including IQ loss and addiction is enormously important to public health and is recommended for immediate further study. Fortifying refined grain and drinking water with biologically available magnesium to pre-twentieth century levels is recommended.
Magnesium (Mg) is an essential element for the body. It is a cofactor for ATP, DNA, and RNA and more than 600 enzymes. As it is similar to Ca2+, this element can also act as a cell signaling molecule and play multiple important roles in the nervous, muscle, and immune systems. Recent studies have associated Mg-deficiency with many neurological disorders, such as cerebral vasospasm, Alzheimer’s disease, stroke, and migraine. As it plays such a crucial role in human body, therefore, we summarized the role of Mg in neurological disorders to illustrate the symptoms caused by Mg-deficiency and the possible underlying mechanisms.
METHODS:
We critically discuss the role of it that we review the recent literature of magnesium. We also review the available data which are concerning the role of magnesium in neurological disorders.
RESULTS:
Magnesium is related to neurological disorders on the basis of the study of animals and humans experiments. Furthermore, these nervous systems related diseases include cerebral vasospasm, Alzheimer’s disease, Parkinson’s disease, stroke and migraine.
CONCLUSION:
Magnesium has effects on neurological disorders, such as its utility in cerebral vasospasm, Alzheimer’s disease, Parkinson’s disease, stroke and migraine. So here we make a brief review to conclude it.
Magnesium is the fourth most abundant mineral in the body. It has been recognized as a cofactor for more than 300 enzymatic reactions, where it is crucial for adenosine triphosphate (ATP) metabolism.
Magnesium is required for DNA and RNA synthesis, reproduction, and protein synthesis. Moreover, magnesium is essential for the regulation of muscular contraction, blood pressure, insulin metabolism, cardiac excitability, vasomotor tone, nerve transmission and neuromuscular conduction.
Imbalances in magnesium status-primarily hypomagnesemia as it is seen more common than hypermagnesemia-might result in unwanted neuromuscular, cardiac or nervous disorders.
Based on magnesium’s many functions within the human body, it plays an important role in prevention and treatment of many diseases. Low levels of magnesium have been associated with a number of chronic diseases, such as Alzheimer’s disease, insulin resistance and type-2 diabetes mellitus, hypertension, cardiovascular disease (e.g., stroke), migraine headaches, and attention deficit hyperactivity disorder (ADHD).
Numerous studies have linked severe stress to the development of major depressive disorder (MDD), and suicidal behaviors.
Furthermore, recent preclinical studies from our laboratory and others have demonstrated that in rodents, chronic stress and the stress hormone cortisol has caused oxidative damage to mitochondrial function and membrane lipids in the brain.
Mitochondria play a key role in synaptic neurotransmitter signaling by providing adenosine triphosphate (ATP), mediating lipid and protein synthesis, buffering intracellular calcium, and regulating apoptotic and resilience pathways.
Membrane lipids are similarly essential to central nervous system (CNS) function, because cholesterol, polyunsaturated fatty acids, and sphingolipids form a lipid raft region, a special lipid region on the membrane that mediates neurotransmitter signaling through G-protein coupled receptors and ion channels.
Low serum cholesterol levels, low antioxidant capacity, and abnormal early morning cortisol levels are biomarkers consistently associated with both depression and suicidal behaviors.
In this review, we summarize the manner in which nutrients can protect against oxidative damage to mitochondria and lipids in the neuronal circuits associated with cognitive and affective behaviors.
These nutrients include ω3 fatty acids, antioxidants (vitamin C and zinc), members of the vitamin B family (Vitamin B12 and folic acid) and magnesium. Accumulating data have shown that these nutrients can enhance neurocognitive function, and may have therapeutic benefits for depression and suicidal behaviors. A growing body of studies suggests the intriguing possibility that regular consumption of these nutrients may help prevent the onset of mood disorders and suicidal behaviors in vulnerable individuals, or significantly augment the therapeutic effect of available antidepressants. These findings have important implications for the health of both military and civilian populations.
The aim of this study was to assess the severity of depressive symptoms in postmenopausal women, depending on serum Mg and Zn levels.
The study involved 171 postmenopausal women from Poland, who were not using menopausal hormone therapy (MHT). The intensity of depressive symptoms was evaluated using a standard research technique, the Beck Depression Inventory (BDI).
The plasma Mg and Zn concentrations were measured. Depressive symptoms of different severity levels were diagnosed in 36.8 % of the women. The mean serum Mg level was 1.53 ± 0.28 mg/dL, and Zn level was 72 ±14 μg/dL.
The women with higher serum Mg and Zn levels had less depressive symptoms, and this observation is a precious information which can be used when planning depressive disorder prevention programmes.
Addiction is a dysregulation of brain reward systems that progressively increases, resulting in compulsive drug use and loss of control over drug-taking.
Addiction is a brain disease.
There is evidence that magnesium deficit is involved in addiction to various addictive substances (heroin, morphine, cocaine, nicotine, alcohol, caffeine, and others). Magnesium is involved in all the stages of addiction. Magnesium deficit enhances the vulnerability to psychoactive substance addiction. Stress and trauma reduce the brain magnesium level and at the same time favor addiction development.
In experimental studies, administration of magnesium while inducing morphine dependence in rats reduced the dependence intensity. Magnesium reduces the NMDA receptor activity and the glutamatergic activity. Because stress and trauma induce hypomagnesemia with increased vulnerability to addiction, magnesium intake by people who are under prolonged stress could be a way to reduce this vulnerability and the development of addiction to different psychoactive substances.
Anxiety and depression appear to be associated with increases in drug-related harm and addictive substance use. Magnesium anxiolytic effect could be important for the antiaddictive action. Addiction is characterized by relapses. Magnesium deficiency may be a contributing factor to these relapses.
To study the efficacy and tolerability of 1 g of intravenous magnesium sulfate as acute treatment of moderate or severe migraine attacks.
BACKGROUND:
Migraine is a common disorder in which not only the pain but also the accompanying symptoms such as nausea and vomiting reduce activity and productivity of sufferers. Many drugs used for the treatment of acute migraine attacks have many side effects, are not well tolerated, are ineffective in some patients, or cannot be used during pregnancy or in patients with ischemic heart disease. Magnesium deficiency has been proposed to play a role in the pathophysiology of migraine, and recently treatment of migraine with magnesium has gained considerable interest.
METHODS:
This was a randomized, single-blind, placebo-controlled trial including 30 patients with moderate or severe migraine attacks. Fifteen patients received 1 g intravenous magnesium sulfate given over 15 minutes. The next 15 patients received 10 mL of 0.9% saline intravenously. Those in the placebo group with persisting complaints of pain or nausea and vomiting after 30 minutes also received 1 g magnesium sulfate intravenously over 15 minutes. The patients were assessed immediately after treatment, and then 30 minutes and 2 hours later. Intensity of pain, accompanying symptoms, and side effects were noted.
RESULTS:
All patients in the treatment group responded to treatment with magnesium sulfate. The pain disappeared in 13 patients (86.6%); it was diminished in 2 patients (13.4%); and in all 15 patients (100%), accompanying symptoms disappeared. In the placebo group, a decrease in pain severity but persisting nausea, irritability, and photophobia were noted in 1 patient (6.6%). Accompanying symptoms disappeared in 3 patients (20%) 30 minutes after placebo administration. All patients initially receiving placebo were subsequently given magnesium sulfate. All of these patients responded to magnesium sulfate. In 14 patients (93.3%), the attack ended; in 1 patient (6.6%), pain intensity decreased; and in all 15 patients (100%), accompanying symptoms disappeared. Both the response rate (100% for magnesium sulfate and 7% for placebo) and the pain-free rate (87% for magnesium sulfate and 0% for placebo) showed that magnesium sulfate was superior to placebo. Twenty-six patients (86.6%) had mild side effects which did not necessitate discontinuing treatment during magnesium sulfate administration.
CONCLUSION:
Our results show that 1 g intravenous magnesium sulfate is an efficient, safe, and well-tolerated drug in the treatment of migraine attacks. It is possible that magnesium sulfate could be used in a broader spectrum of patients than other drugs commonly used for attack treatment. In view of these results, the effect of magnesium sulfate in acute migraine should be examined in large-scale studies.
Depression is common, places a large burden on the patient, their family and community, and is often difficult to treat.
Magnesium supplementation is associated with improved depressive symptoms, but because the mechanism is unknown, it is unclear whether serum magnesium levels act as a biological predictor of the treatment outcome.
Therefore, we sought to describe the relationship between serum magnesium and the Patient Health Questionnaire (PHQ, a measure of depression) scores. A cross-sectional analysis of medical records from 3604 adults (mean age 62 years; 42% men) seen in primary care clinics between 2015 and 2018, with at least one completed PHQ were included.
The relationship between serum magnesium and depression using univariate analyses showed a significant effect when measured by the PHQ-2 (−0.19 points/mg/dL; 95% CI −0.31, −0.07; P = 0.001) and the PHQ-9 (−0.93 points/mg/dL; 95% CI −1.81, −0.06; P = 0.037).
This relationship was strengthened after adjusting for covariates (age, gender, race, time between serum magnesium and PHQ tests, and presence of diabetes and chronic kidney disease) (PHQ-2: −0.25 points/mg/dL; 95% CI −3.33, −0.09; P < 0.001 and PHQ-9: −1.09 95% CI −1.96 −0.21; P = 0.015).
For adults seen in primary care, lower serum magnesium levels are associated with depressive symptoms, supporting the use of supplemental magnesium as therapy. Serum magnesium may help identify the biological mechanism of depressive symptoms and identify patients likely to respond to magnesium supplementation.
Type 2 diabetes mellitus is a major global public health problem in the worldwide and is increasing in aging populations. Magnesium intake may be one of the most important factors for diabetes prevention and management. Low magnesium intake may exacerbate metabolic abnormalities. In this study, the relationships of magnesium intake with metabolic parameters, depression and physical activity in elderly patients with type 2 diabetes were investigated.
Methods
This cross-sectional study involved 210 type 2 diabetes patients aged 65 years and above. Participants were interviewed to obtain information on lifestyle and 24-hour dietary recall. Assessment of depression was based on DSM-IV criteria. Clinical variables measured included anthropometric measurements, blood pressure, and biochemical determinations of blood and urine samples. Linear regression was applied to determine the relationships of magnesium intake with nutritional variables and metabolic parameters.
Results
Among all patients, 88.6% had magnesium intake which was less than the dietary reference intake, and 37.1% had hypomagnesaemia. Metabolic syndromes and depression were associated with lower magnesium intake (p < 0.05). A positive relationship was found between magnesium intake and HDL-cholesterol (p = 0.005). Magnesium intake was inversely correlated with triglyceride, waist circumference, body fat percent and body mass index (p < 0.005). After controlling confounding factor, HDL-cholesterol was significantly higher with increasing quartile of magnesium intake (p for trend = 0005). Waist circumference, body fat percentage, and body mass index were significantly lower with increase quartile of magnesium intake (p for trend < 0.001). The odds of depression, central obesity, high body fat percentage, and high body mass index were significantly lower with increasing quartile of magnesium intake (p for trend < 0.05). In addition, magnesium intake was related to high physical activity level and demonstrated lower serum magnesium levels. Serum magnesium was not significantly associated with metabolic parameters.
Conclusions
The majority of elderly type 2 diabetes who have low magnesium intake may compound this deficiency with metabolic abnormalities and depression. Future studies should determine the effects of increased magnesium intake or magnesium supplementation on metabolic control and depression in elderly people with type 2 diabetes.
Sixty percent of cases of clinical depression are considered to be treatment-resistant depression (TRD). Magnesium-deficiency causes N-methyl-d-aspartate (NMDA) coupled calcium channels to be biased towards opening, causing neuronal injury and neurological dysfunction, which may appear to humans as major depression.
Oral administration of magnesium to animals led to anti-depressant-like effects that were comparable to those of strong anti-depressant drugs. Cerebral spinal fluid (CSF) magnesium has been found low in treatment-resistant suicidal depression and in patients that have attempted suicide. Brain magnesium has been found low in TRD using phosphorous nuclear magnetic resonance spectroscopy, an accurate means for measuring brain magnesium. Blood and CSF magnesium do not appear well correlated with major depression.
Although the first report of magnesium treatment for agitated depression was published in 1921 showing success in 220 out of 250 cases, and there are modern case reports showing rapid terminating of TRD, only a few modern clinical trials were found.
A 2008 randomized clinical trial showed that magnesium was as effective as the tricyclic anti-depressant imipramine in treating depression in diabetics and without any of the side effects of imipramine. Intravenous and oral magnesium in specific protocols have been reported to rapidly terminate TRD safely and without side effects.
Magnesium has been largely removed from processed foods, potentially harming the brain.
Calcium, glutamate and aspartate are common food additives that may worsen affective disorders.
We hypothesize that – when taken together – there is more than sufficient evidence to implicate inadequate dietary magnesium as the main cause of TRD, and that physicians should prescribe magnesium for TRD.
Since inadequate brain magnesium appears to reduce serotonin levels, and since anti-depressants have been shown to have the action of raising brain magnesium, we further hypothesize that magnesium treatment will be found beneficial for nearly all depressives, not only TRD.
ChooseLife : Has there ever been a more important time to eat your greens? Make Green Smoothies? Take Epsom Salts baths? or, a few grains of Epsom Salts in drinking water through the day?