The spleen is my favourite organ in the body. As an acupuncturist, I am not
really supposed to play favourites, saying you love one organ more than the
others is like a parent declaring that they love one of their children more,
but I feel like I have a special connection with the spleen. I talk about it a
lot and I seem to write about it even more. It is a hard working and often
under appreciated little organ, so it is my duty, and my privilege to give it
some much needed love and attention.
The spleen is an organ that doesn’t really get discussed very much in relation to the other organs of the body. I think its role in Western medicine is perhaps seen as less ‘vital’ than the other organs, but the role of the spleen in Western medicine is very different than its role in Chinese medicine.
The Spleen In Western Medicine
In Western medicine the spleen is part of the immune system and the largest organ in the lymphatic system. It is where red blood cells are recycled and where white blood cells, called lymphocytes, are stored. It is possible to live without a spleen. You can lacerate or rupture your spleen in a car accident or playing contact sports (or via any severe physical trauma) and the spleen may have to be repaired or removed completely (called a splenectomy). Although it is possible to live without a spleen because other organs overcompensate and take over many of its important functions, it makes a person more susceptible to infections and ultimately compromises their immune system.
The Spleen In Chinese Medicine
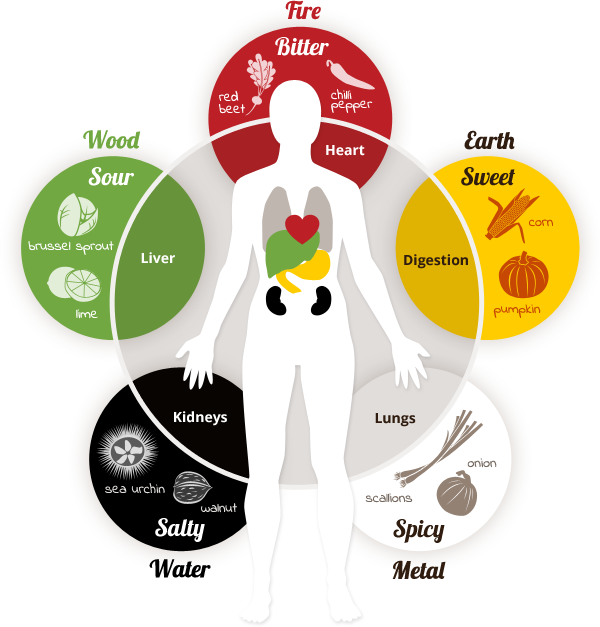
This lovely image is from thespicedoc.com and designed by Patricia Callison
The spleen has a fundamental role in Chinese medicine. It, paired with the stomach, are the main organs of digestion and are responsible for digestion and distribution of food and nutrients throughout the body. The spleen extracts qi from the food we eat that is used by the body to build immunity (wei qi), keep things moving freely (stagnation leads to disease), the proper functioning of the other organs and helps to regulate mental functions and emotions.
Why Our Culture Is Hard On The Spleen
It is very common in our culture to have a deficiency of the spleen. Because the spleen is the main organ of not only digestion, but processing, it is responsible for processing the food and drink that we consume, as well as all of the stimulus that comes in through our sense organs. We are a culture that values doing many things at once. The more productive we can be, the more we are praised at our jobs and in life. This philosophy is contrary to the health of the spleen. In Chinese medicine, to keep the spleen healthy, it is important to do one thing at a time, and as mindfully as possible. The idea is that the spleen is then able to use all of its energies to process one thing, rather than having to process many things at once, which wipes out its energy stores, or spleen qi. Examples of doing many things at once are eating (taking in food/drink) while watching TV (taking in stimulus). Or eating while sitting at your computer working. These are commonplace in a culture where everyone has too much to do and is always short on time. This is one of the biggest reasons that so many people suffer with a deficiency of their spleen qi. So, do one thing at a time. If you are going to eat, just eat. Really concentrate and be mindful about what you are doing. Enjoy and savour your food, this will not only help your spleen, but lead you to be more relaxed and help you digest more efficiently too.
A Strong And Balanced Spleen
People with strong and balanced spleen energy have the following
characteristics:
responsible
practical
hard working
strong
like to nurture themselves and others
active
stable
excellent endurance
good appetites
good, healthy digestions
strong limbs
are orderly and careful
often very creative
have fertile imaginations
A Spleen Imbalance
People with an imbalance of their spleen often display the following
characteristics:
chronically tired
a feeling of being “stuck”
in their lives
physical and/or mental
stagnation
weak digestion (lots of
digestive issues)
poor appetite
diminished sense of taste
loose stools
abdominal bloating and
tenderness
masses in the abdomen
weight problems (either
overweight without overeating or underweight without the ability to gain)
Spleen Qi Deficiency
A deficiency of spleen qi can be caused by many things. Eating a poor diet
of mostly refined, highly processed foods where the body is not receiving
enough nourishment is certainly common, especially in industrialized nations
where foods tend to be overly processed and many people make poor food choices.
Another cause is simply our hectic lifestyles. As I mentioned above, we are a
culture of multitasking, and this is particularly hard on the tiny organ that
is responsible for doing all the processing. If it is constantly overloaded,
then it will become exhausted, leading to spleen qi deficiency. Another cause,
and this is also extremely common, is the emotional aspect of the spleen. In
Chinese medicine, every organ is associated with an emotion. An excess of that
emotion can damage the related organ, and likewise, when the organ is out of
balance, it can have a strong effect on the corresponding emotion. The emotion
of the spleen in worry/over thinking. If there is one emotion that I see more
than any other in clinic, it is WORRY. An excess of worry and over thinking, as
well as having a hard time just shutting off your brain, is damaging to the
spleen. And we do that so much in our society. The pressures on us are
enormous, and people are simply overworked and overstressed. So, poor
nutrition, multitasking and a propensity to worry are all part of our culture,
and all are affecting our poor, overworked spleens. It’s no wonder spleen qi
deficiency is so common.
Here are some symptoms of spleen qi deficiency so you know what to look for:
weakness of the whole body
fatigue
loose stools with
undigested food
a pale tongue with a thin
white coat and teeth marks on the sides
a weak pulse
weakness of the arms and
legs
weak muscles
prolapse of organs (such as
hemorrhoids, uterus, bladder, intestines)
The symptoms above all point to a spleen imbalance. There is good news though. There is wonderful nutritional therapy for deficient spleen qi, and as many Chinese doctors have known for centuries, food is the best medicine.
The Thermal Nature Of Foods In Chinese Medicine
When we talk about nutritional therapy in Chinese medicine, which is an important modality, we talk about the thermal nature of foods. This can be a bit of a difficult concept to understand at first, but once it’s explained, it actually starts to make a lot of sense. Thermal nature is not just how physically cold or hot a food is as a result of cooking. In Chinese medicine, all foods are seen to have a fundamentally thermal nature, either warming, cooling or neutral, and these are important to know as they have a direct effect on the body. In the context of Chinese medicine it is also important to know the thermal nature of your body, which is measured by the relative yin and yang energies it encompasses. For example, if a person comes to you with a red face, bloodshot eyes, outbursts of anger and is shouting, it is pretty safe to determine that that person has an excess of yang energy and thus, should eat cooling foods and stay away from warming ones until the balance of yin and yang is reestablished. Every organ also, has a temperature that it prefers, so it is good to know all these things when thinking about food therapy in terms of health and disease.
Food Therapy For Spleen Qi Deficiency
With foods thermal nature in mind, the spleen likes to be warm and dry. So
if you have spleen qi deficiency, you want to eat foods that are warming, or at
least neutral to help build the spleens energy. Cold foods should be avoided as
they weaken digestion. Also, foods that are cold in temperature take more
energy for the spleen to digest and are seen to extinguish the digestive fire.
The flavour associated with the spleen is sweet, so as a rule, sweet foods are
prescribed to correct a deficiency.
One of the best foods to build spleen qi is cooked white rice, often eaten in the form of congee or jook. Congee is essentially a porridge made of overcooked rice and water. You may add other ingredients depending on your condition and taste. For spleen qi deficiency or any weakness of the spleen, warming ingredients would be appropriate. See the list below.
Beneficial Spleen Foods
Vegetables
pumpkin
yam
black beans
garbanzo beans
carrot
parsnip
squash
peas
sweet potato
onion
leek
Spices
black pepper
ginger
nutmeg
cinnamon
fennel
garlic
Sweeteners (in small amounts)
barley malt
rice syrup
molasses
cherries
dates
Animal Products (if the deficiency is severe)
mackerel
tuna
halibut
anchovy
beef
beef liver or kidney
turkey
chicken
lamb
butter
Chewing foods well is also important when spleen energy is weak. This helps to break down foods before they get to the spleen and means the spleen has less work to do and conserve its energy. Eating things like soups are beneficial because they are cooked until soft and are less work for the spleen to digest. And finally, the preparation of food is also a factor in helping to build up spleen qi. Eating on the run and eating out mean that you are not taking the time and intention to mindfully prepare the foods that you are eating. To prepare foods with care infuses them with healing energies that the whole body, and especially the spleen, needs. So take the time to prepare the foods that you are eating with love, your spleen will appreciate it. 🙂
David Carr, M.D., from University of California in San Diego, and H. Gilbert Welch, M.D., a general internist in Thetford, Vermont, used the Open Payments database to determine industry payments made to physician directors of NCI-designated cancer centers (2015 through 2017).
The researchers found that of the 53 physician cancer center directors listed in 2017, 44 held the position in 2016 and 41 in 2015. In 2017, payments totaled $4.42 million, including $1.89 million in research payments to 12 directors and $2.53 million in nonresearch payments to 22 directors. Half of directors (51 percent) received no payments, while more than one-third (36 percent) received more than $5,000. Physician directors were more likely to receive payments unrelated to research than they were to receive research payments, with 12 of the 53 directors receiving payments unrelated to research exceeding the $5,000 threshold (defined as a significant financial interest by the NCI) and two receiving payments of more than $50,000. In 2017, 12 directors received research payments, with four receiving more than $50,000.
“Our findings raise the question of whether industry payments to the directors of publicly supported institutions, such as NCI-designated cancer centers, serve the public interest,” the authors write.
The books of Dr. Lobsang Rampa have introduced many thousands of people in the west to buddhist teachings and spiritual and metaphysical knowledge. Dr. Rampa was amongst the first eastern teachers to make this knowledge accessible to westerners in an easily understandable and enjoyable format and a forerunner of today’s buddhist teachers such as Sogyal Rinpoche and Ringu Tulku.
Dr. Rampa was a prolific author – his first book “The Third Eye” published in 1955, was followed by 23 more, and he continued to write until shortly before his death in Canada in 1981.
Why not read one and investigate Dr. Rampa’a writings for yourself? This page gives an outline of the content of many of the Rampa books and gives extracts to get a flavour of the books.
Selection of books by Dr. Tuesday Lobsang Rampa – free downloads:
Click to view online in a separate window, or right-click and choose “save target as” to download to your computer. The files are in Word format and are between 600k and 1.1Mb in size.
A Comparison of Primitive and Modern Diets and Their Effects.
Chapter 17 : Origin Of Physical Deformities
One origin of physical deformities
FACES are classified on the basis of physical characteristics and appearances which identify them as having a common ancestry. The constant reproduction of ancestral patterns constitutes one of the fundamental laws of heredity. We are concerned here with the divergences from the normal course of reproduction.
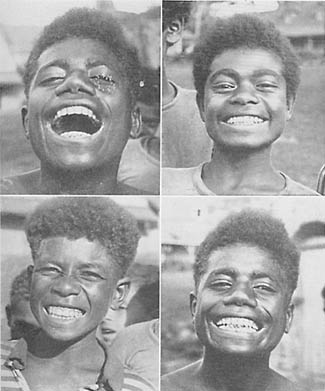
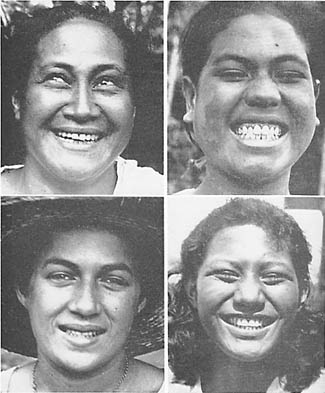
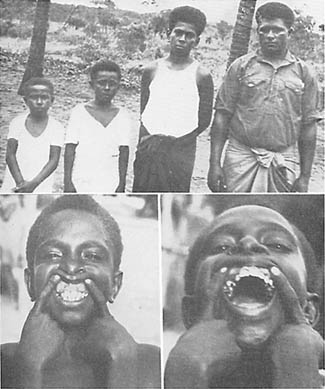
The precision with which Nature reproduces widely distributed racial stocks demonstrates how deeply seated and controlling are the Mendelian laws. In Fig. 98 may be seen four young men of the Melanesian race born on four different islands. They have never seen each other, yet they look like brothers. Similarly, in Fig. 99 are shown four Polynesian girls. Here again they look so much alike that they might readily be taken for sisters. Yet, they live in four different groups of Polynesian islands; the Hawaiian, the Samoan, the Tahitian, and the Rarotongan.
FIG. 98. These four Melanesian boys born on different islands look like brothers but are not blood relations. They illustrate the role of heredity in reproducing racial type. Heredity, however, can only operate normally when the germ cells have not been injured. 99. These four Polynesian girls live on different islands and are not related though they look like sisters. They record their racial type by undisturbed heredity
The blending of different racial stocks produces typical characteristics of either or both ancestral patterns. When, however, marked divergences appear without mixing of racial stocks, the result is not due to heredity, but occurs in spite of heredity. In the previous chapters, I have shown that in the modernized groups of various primitive racial stocks, ccrtain individuals developed marked changes in facial and dental arch form from the racial pattern. We are interested to know the nature of the forces responsible for this distortion of the ancestral pattern. In a study of 1,276 skulls of the ancient civilizations of Peru, I did not find one with a typical divergence from normal such as we find in modern whites or in children of primitive racial stocks after the parents have adopted the foods of our modern civilization. It is important that we study this phase in further detail.
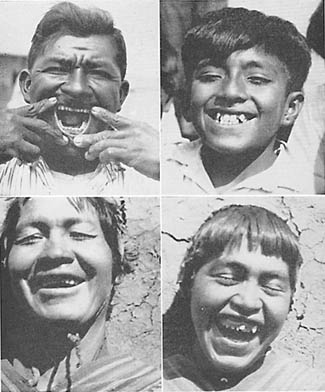
In Fig. 100 are shown two Indian fathers and their sons, whom we studied in Peru. The father and son shown above lived at Talara, in a highly modernized Indian colony. The father worked in the oil fields on the coast. This district is an arid desert into which practically all food has to be shipped for the large colony engaged in the oil industry. The father was born while his parents were using the native foods of the coast, including an abundance of sea foods. The son was born to his parents after they had adopted the foods of modern civilization. The father and son shown below, lived in the high Sierras. The father is an Indian descendant of the Incas and was born while his parents were living on the native dietary of the high plateau country, near Cuzco. After the adoption of the modern foods by the parents, the son shown to the right was born. It is important to keep in mind that the marked change in these fathers and sons has occurred in the first generation after the parents have adopted the white man’s foods, and has occurred in spite of heredity.
FIG. 100. Disturbed heredity. Above, father a primitive coastal Indian of Peru with normal facial and dental arch development. Son at right presents distortions of both facial and dental arch form. Below, father a primitive Andean Indian with excellent facial and dental arch form. His son at right has not reproduced the racial pattern. Both sons are full blood.
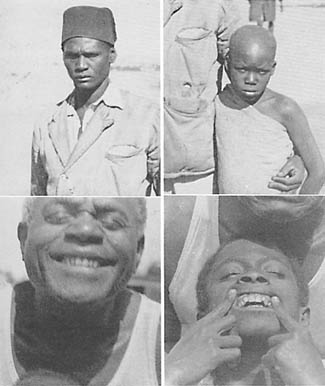
In Fig. 101 above is shown a Wakamba father in central Africa, a man who is working for the railroad company which contributed largely to the food supply for the laborers. The boy shown at the right was born after the parents had adopted the imported foods. In the lower picture, in Fig. 101, is seen a Fiji Islander and his son. The father was born to parents living on the native foods, and his son was born after the adoption of the white man’s foods. All these are typical cases of the inhibition of Nature’s normal procedure. We have additional data which indicate that our problem is associated with a progressive lowering of reproductive capacity on the part of one or both of the parents.
FIG. 101. Disturbed heredity. Above, the father is a primitive Wakamba of Central Africa. His son at right has not reproduced the tribal pattern. Below, the father presents the typical Fijian primitive facial and dental arch form. His son at right has a narrowed arch and change in facial form. Both sons are full blood.
In photographing the members of modernized families, regardless of racial stocks, we frequently find that changes in facial expression appear in the younger members of the family. This change in facial contour within a family does not occur in the primitive races, while on their native dietary.
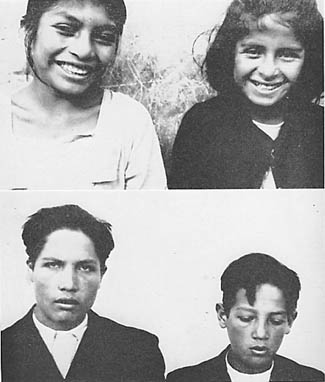
In contrast with this we see, in Fig. 102, two sisters and two brothers. In each pair there is a marked change in the facial form of the younger. The arches and the nostrils of the younger child are narrower and there is a marked lack of development in both the middle and lower thirds of the face.
FIG. 102. Disturbed heredity. Quichua Indians. Note the marked change in shape of the face and dental arches of the younger sister at the right. Also of the younger brother at the right. These families demonstrate a lowering of reproductive capacity of the parents with the later born children.
Very striking illustrations of this progressive degeneration in the children of a given family were found among the modernized aborigines of Australia. Two views of brothers are shown in Fig. 103 (upper). The father and mother of these two boys were born in the Bush. They were living, when photographed, in one of the reservations, on the imported modern foods which were provided by the government. This is also illustrated in the lower photograph. Note the marked underdevelopment of the middle third of the face of the girl.
FIG. 103. Disturbed heredity. These children are Australian Aborigines. Note the marked change in facial and dental arch form in the younger child at the right in both families. This is depressed reproductive capacity of the parents.
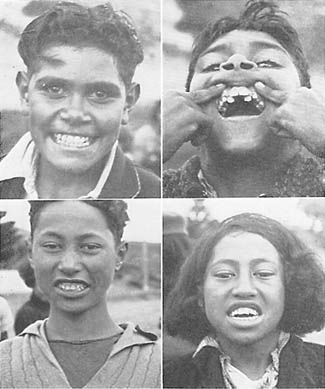
Striking instances were frequently seen among the modernized Maori of New Zealand. Two sisters presenting two extremes of facial form are shown in the upper section of Fig. 104. The girl to the left is the older. She has the typical tribal pattern which has been completely lost in her younger sister to the right.
FIG. 104. Above, two Maori girls in New Zealand and below, two white girls in Peru. Note the facial change in the girls at the right compared with their older sisters.
If the change in facial form were the result of racial admixture, we should not have the types of deformity patterns that these cases show. Indeed, in the same family we should not find several different deformity patterns. The lack of development downward of the upper anterior incisors and the bone supporting them is illustrated for the younger child, in Fig. 103 lower right. It will be noted that when this girl’s molar teeth are in contact her front teeth still miss occluding by a considerable distance.
Members of the white race are affected in a similar manner. In Fig. 104 (lower) are shown two sisters; the younger to the right reveals strikingly the lack of development of the middle and lower third of the face. The fact that this condition so frequently shows a progressively severe injury in the younger members of the family is a matter of great importance in tracing the causative factors. It is important to keep in mind that when the injury shows in the face of the young child it becomes worse when the adult face forms. This increase in deformity occurs at the time of the development of the permanent dentition, at from ten to fourteen years of age.
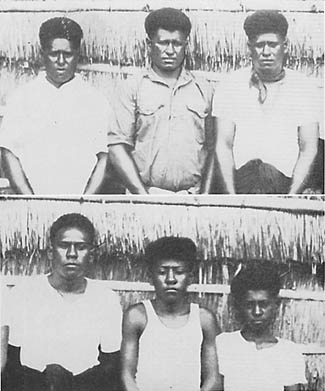
In the islands north of Australia where contact with modern civilization is just being made, the adult individuals showed a constant reproduction of the tribal pattern, while those born since contact was made, had many divergences from normal. In Fig. 105 will be seen a family of six individuals. Four were born before the modern store was put on that island and two after the parents had come into contact with the influence of the imported foods. It will be seen that the four older brothers show marked uniformity of facial design, and that all have reproduced the tribal pattern. The two younger members show definite change in facial pattern. This is also illustrated in Fig. 106 above, in which the oldest brother was born before the store was put on Badu Island, and the three younger, after the establishment of the store twenty-three years ago.
FIG. 105. Of these six brothers the four older were born on Badu Island before the white man’s store was established. The two younger at right below, after. Note change in facial form. FIG. 106. Above, the brother at the right was born before the store was put on Badu Island, the three younger, after. Note the change in facial form. Below, note that the dental arches are too constricted to provide space for the erupting cuspids. This boy is the one shown at the left in Figure 107.
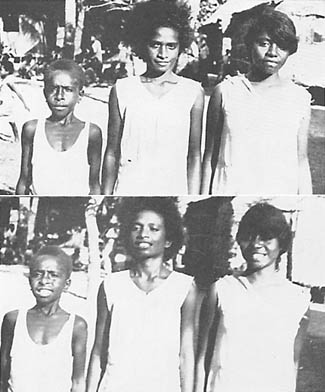
This problem of progressive degeneration in the younger members of the family is again illustrated by the group shown in Fig. 107. The older girl has reproduced the tribal pattern of the race with normal broad, dental arches. The second girl shows marked narrowing and lengthening of the face. The third child, a boy, shows very marked divergence from the tribal pattern. This group is shown below with their teeth exposed. It will be seen that the oldest girl has broad dental arches typical of Nature’s normal design. The second girl has a marked depression laterally in the molar and bicuspid region producing a narrowing of the palate. The third child has in addition to the narrowing of the face a marked deficiency in bone growth so that the cuspids both above and below are forced entirely outside the arch. The total circumference as well as the breadth of the upper arch is so reduced that space is not available for the cuspids. They will be seen imbedded high in the tissue, as illustrated in the lower picture of Fig. 106.
FIG. 107. Natives from islands north of Australia. Above, note the progressive facial change in the younger sister and brother with lengthening and narrowing of the face and body. Below, note the broad arches of the oldest girl at the right, lateral depression of the bicuspids and molars of the next girl and inadequate bone development of the boy’s face. These are on an island north of Australia.
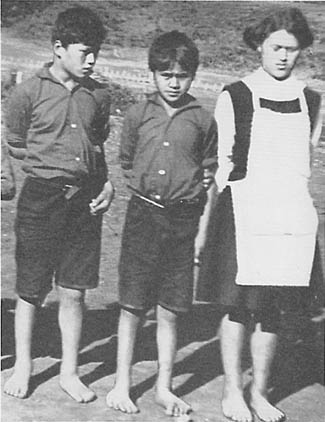
Fig. 108 shows three white girl scouts in New Zealand. Note that progressive narrowing of the body including both shoulders and hips has occurred in the younger members of the family. This is also shown in Fig. 107.
FIG. 108. White Girl Scouts, New Zealand. Note the progressive lengthening and narrowing of the face and narrowing of the hips in the younger girl at the left.
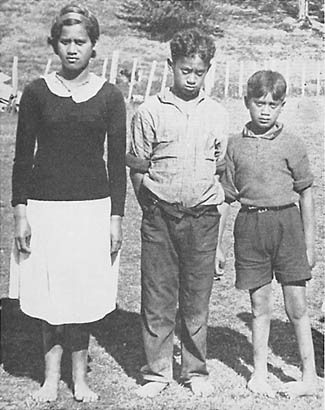
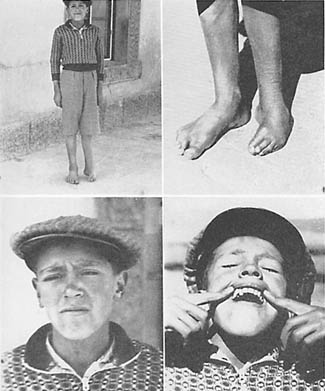
It would be remarkable if these disturbances in the physical pattern were limited to the face and dental arches. An illustration of other deficiency injuries is shown in Fig. 109, which shows three children in a modernized Maori family. It will be seen that while the oldest girl has the typical Maori racial pattern of face, there is a marked lack of development of the middle third of the face, with progressive severity of distortion in her two younger brothers. On observing the feet it will be seen that she has splendidly formed feet while the second child has flat feet, and the third child has clubbed feet.
FIG. 109. New Zealand Maori. Note the progressive change in facial form of the two younger boys as compared with their older sister. Then note the progressive change in their feet. Normal feet, flat feet and club feet.
I have found similar examples in several of the modernized primitive racial stocks. The severity of the disturbing factors may be different under different circumstances. Drought, industrial depression, unemployment, and the like, all have their influence. In Fig. 110 will be seen three Maori children of New Zealand; the second child is smaller in stature than the third and gives more evidence of facial injury. While his older sister and younger brother have normal feet, his quite severe disturbance in facial growth is associated with club feet.
FIG. 110. New Zealand Maori. Note the marked undersize of the second child and underdevelopment of the face associated with marked deformity of the feet.
I have one patient who was the seventh of a family of eleven children. All the children in the family have good facial development, except this patient. She was born in the midst of a severe financial depression when the total amount of money available for the food for the family was reduced to a very low level. The other children were born before or after the depression, and were not injured. In addition to this patient’s severe facial deformity, she has had some arthritis and a general rheumatic tendency. Her facial injury is marked and is characterized by a lack of development of the middle third.
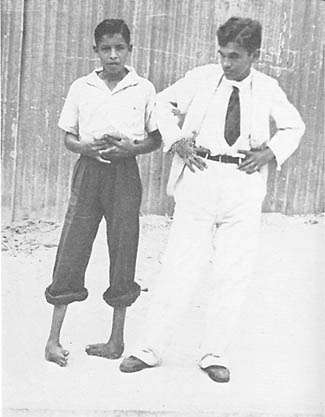
Deformities of the feet associated with facial deformity have been found in several modernized groups of primitive racial stocks. A typical case among the modernized Indians of Peru is shown in Fig. 111. The face of this boy shows abnormal development with narrowing of the upper arch and displacement of the teeth. This is associated with gross deformity of one foot and shortening of the leg. He lives in the high country. This phase is strikingly illustrated in Fig. 112 where the face is very badly injured and both feet are seriously clubbed. This boy is a Coastal Indian.
FIG. 111. This boy is a modernized Indian in the high Sierra of Peru. Note the disturbed development of the face associated with the deformity of one foot. FIG. 112. This is a modernized coastal Indian of Ecuador. Note the serious facial and dental arch distortion associated with club feet.
The serious expressions of physical deformities which we found had occurred in several primitive racial stocks, after they have become modernized sufficiently to be using the foods of our modern civilization, are occurring in our modern American families with equal severity and great frequency.
One method for determining the cause of these deformities is through an examination of birth and death certificates to note the recorded data relative to physical deformities. An outstanding contribution to this approach has been made by Dr. D. P. Murphy, of the University of Pennsylvania. In an examination of 130,132 individual death certificates that have been recorded between 1929 and 1933, he found physical deformities recorded in 1,476 cases. Dr. Murphy sent field workers to make a personal study of the family histories by contacting the mothers or grandmothers, of whom they were able to locate 890. From this group he was able to select 405 with sufficiently complete family histories to allow tabulation in a form that would throw light upon the birth rank and other data. His studies strongly emphasize the presence of a period of low reproductive activity. In concluding one of his reports he states: (1)
Miscarriages, stillbirths, and premature births occurred more often than would be expected by chance in the pregnancies immediately preceding and immediately following the pregnancy which resulted in the birth of a defective child, and less often than would be expected by chance in the remaining pregnancies. Miscarriage, stillbirth, and premature birth occurred most often in the pregnancy immediately preceding that of the defective child.
From the above observations, it is concluded that the birth of a congenitally malformed child may be only one expression of a prolonged decrease in functional reproductive activity, the other expressions being miscarriages, stillbirths, and premature births.
It is suggested that the obstetrician has unusual reason to suspect the possible existence of a congenital malformation in the pregnancy which follows immediately after a miscarriage, a stillbirth, or a premature birth.
Shute, of the University of Western Ontario, London, Canada, in a personal communication, states that he has been impressed, in his studies of aborted fetuses, with the large percentage that are malformed. This seems to link the malformations with the causative factors which have resulted in decreased reproductive activity.
In connection with the production of imperfect infants, the period in the formative process at which the injury occurs and also its origin are important. Murphy has thrown important light on this phase in his study of the cause of the defectives in forty families with two or more malformed. (2) He concludes: “Many if not most of the congenital malformations met with in this study resulted from defects in the germ plasm, which were present before fertilization.”
Among the important questions that arise is the relative responsibility of the two parents. As an approach to this phase Murphy (2) has made a study which deals with a consecutive series of 884 families in each of which there appeared at least one congenitally malformed child. In forty of these families, there were two or more malformed brothers and sisters. He presents extensive data in tabular form from which he takes examples to illustrate his interpretation. He states under the “Clinical Value of Study” the following:
It is evident from the above data (tables) that there is a strong tendency for congenital malformations to duplicate in siblings that belong to a consecutive series of families. And also that such defects tend to appear rather frequently among their more distant relatives. This duplication of malformations is to be observed in the case of the more serious types of defects, just as it is noticed in the less serious ones. These findings lend support to the theory that congenital malformations are primarily the result of influences which affect the germ cells prior to, rather than after, fertilization. The validity of this theory is emphasized by three examples taken from Tables I and II. Family 17 in Table I contained 3 children with pyloric stenosis, two of which were twins. Family 6 in Table II possessed 2 siblings with cleft palate, conceived by the same father, but born to different mothers. Family 8 in Table II contained 2 children both exhibiting an absence of the right half of the diaphragm. It does not seem likely that such sequences of events as these could be the result of any forces that did not operate until after fertilization had taken place. . . .
Since, as has been shown in a previous report, congenital malformations are 24 times more common in siblings of defective children than in the population at large, the present observations should be of added clinical interest.
Summary and Conclusions
A consecutive series of 40 families having 2 or more congenitally malformed children has been studied with respect to the duplication of defects in siblings.
The defect observed in the first malformed child reappeared in a subsequent malformed sibling in about 50 per cent of all cases; the 50 per cent remaining including all other possible defects.
In a second group of 39 consecutive families, in which a malformed child possessed a malformed relative, the malformation in the child and in the relative were identical in about 41 per cent of cases.
In 19 non-consecutive families with 2 or more malformed children, the defect of the first child repeated in a subsequent child in over half of the families.
It is significant that while these important factors are just coming to light in our modernized civilization, the evidence clearly indicates that several so-called primitive races have been conscious of the need for safeguarding motherhood from reproductive overloads which would reduce the capacity for efficient reproduction. For example, G. T. Baden (3) in his book “Among the Ibos of Nigeria” states:
It is not only a matter of disgrace but an actual abomination, for an Ibo woman to bear children at shorter intervals than about three years. . . . The idea of a fixed minimum period between births is based on several sound principles. The belief prevails strongly that it is necessary for this interval to elapse in order to ensure the mother being able to recuperate her strength completely, and thus be in a thoroughly fit condition to bear another child. Should a second child be born within the prescribed period the theory is held that it must inevitably be weak and sickly, and its chances jeopardized.
Similarly, the Indians of Peru, Ecuador and Columbia have been familiar with the necessity of preventing pregnancy overloads of the mother. Whiffen (4) in his book “North-West Amazons” states:
The numbers (of pregnant women) are remarkable in view of the fact that husbands abstain from any intercourse with their wives, not only during pregnancy but also throughout the period of lactation–far more prolonged with them than with Europeans. The result is that two and a half years between each child is the minimum difference of age, and in the majority of cases it is even greater.
It may also be important to note that the Amazon Indians have been conscious of the fact that these matters are related to the nutrition of both parents. Whiffen states that:
These Indians share the belief of many peoples of the lower cultures that the food eaten by the parents–to some degree of both parents–will have a definite influence upon the birth, appearance, or character of the child.
This problem of the consciousness among primitives of the need for spacing children has been emphasized by George Brown (5) in his studies among Melanesians and Polynesians in which he reports relative to the natives on one of the Solomon Islands as follows:
After the birth of a child the husband was not supposed to cohabit with his wife until the child could walk. If a child was weak or sickly, the people would say, speaking of the parents, “Ah, well, they have only themselves to blame.”
These new data have a very important bearing on the problems of degeneration in our modern civilization. Since it is true that a racial pattern can be changed in a single generation our modern concept and teaching with regard to the role of heredity must be modified, in its relationship to cause and effect. A deformity arising from intercepted heredity is just as truly biologic as a deformity arising from accumulated impacts as expressed in heredity. Instead of blaming the past generations for the distortions or frailties of our modern generation and thus relieving our own generation of responsibility these new data indicate that the social organization that is creating these divergencies from normal must alone accept the responsibility.
This completely changes some aspects of the theories and practice of modern social education. Instead of planning the care and management of distorted personality as though the lesion were the result of environmental influences upon a normally organized individual, it should be looked upon as a distortion affecting one link in the chain of heredity which is neither the result of the distortions of previous links nor a controlling factor for future links in the chain. The prognosis, in other words, while being bad for the individual is not necessarily bad for his or her descendants.
While many of the individuals who have suffered physical distortions have apparently practically normal brain development we shall see in the following chapter that a certain percentage have so great a disturbance in brain organization that they cannot and should not be considered as individually responsible for their behavior.
It is urgent therefore that the data presented in this chapter be looked upon as an important key to the progressive degeneration that is taking place in many parts of the world under the influence of our so-called modern civilization. It is a matter of profound significance that the most primitive races were originally able to avoid the physical degeneration so general in many communities today. It is also a matter of importance that the primitives recognized not only these dangers but were conscious of and practiced adequate means for preventing them. They had sufficient character to achieve the ends which they deemed essential. Weakness in character may constitute the greatest barrier in the reorganization and conservation of our modern civilization.
Two serious defects from which many individuals in our modernized civilization suffer are impacted teeth and the absence of teeth due to their failure to develop. It is significant that in the arches of the primitive races practically all teeth form and erupt normally, including the third molars. In the modernized primitives and among our modern whites with deformed dental arches many teeth are impacted and often several of the permanent teeth have never formed. The evidence indicates that this, like the facial and dental arch deformities is due to an absence of vitamin A in the diet of the mother during the gestation period or of one or both of the parents prior to conception. The cause is discussed in the next chapter.
References
MURPHY, D. P. Reproductive efficiency and malformed children. Surg. Gynec. and Obst., 62:585, 1936.
MURPHY, D. P. The duplication of congenital malformations in brothers and sisters and among other relatives. Surg. Gynec. and Obst., 63:443, 1936.
BADEN, G. T. Among the Ibos of Nigeria. Phila., Lippincott, 1921.
WIFFEN, T. North-West Amazons. N. Y., Duffield, 1915.
BROWN, G. Melanesians and Polynesians. London, Macmillan, 1910.
ChooseLifeNotes : Here is the full book, online version – Full Book Please check your own area for copyright information.
PREFACE: To “My Dear friends of Nature and to those people seeking happiness. M.T. I write to you today as MatteoTavera.
I wish to be brief and non–invasive as I offer you my work, the fruit of numerous years of reflections and observations. It took a long time to study and discuss my observations with Nature and to reach this hypothesis. Suddenly, one day a great enlightenment happened to me in full clarity.
Having discovered this truth, I cannot detach it from my spirit since Nature, in its total beauty, is more generous to me now that I finally understand it. Nature no longer teases me about its constant work, its rights and obligations engendered within. Now that I understand it, Nature reveals itself totally, and the intrigue becomes challenging.
LA MISSION SACREE, (SACRED MISSION) is the hypothesis on which I found my law. I present it to you, my dear Friend of Nature, today, for your pleasure, for your health, for the Earth and of all of its fruits. In addition, on this day as I converse with Nature, if you are disposed to take on the relay, I am then certain that many mysteries will also appear before you, just as luminous in total clarity as which occurred to me.
This work is destined to a certain category of persons who love Nature and show interest in the problems of life. As well, it includes those who think that not all is going so well on this earth, certainly not as it should. Who has not echoed a cry of alarm started by Illustrious American Biologist, Raquel Carson in her resounding book: “Silent Spring”? This work carries the introduction of Scientist Jean Rostand, stating “A strong voice calls us to give our help to Nature slowly being assassinated by men” and Roger Heim wrote the preface as director of “Musee National d’Histoires Naturelle” and PRESIDENT OF THE “ACADEMIE DES SCIENCES”. At that exact same time, Günter Schwab in Germany was shouting the same cries in his book: “Dance with the Devil”. The French version of this serious work was recognized in “La Presse” in France and Europe.
Many serious magazines around the world also show their great interest and concern in “Sicknesses of Civilization.” Are they not tired of the excess use of chemical products in the domains of agriculture, industry and food preparations? Besides the number of interested lay people ever increasing, including doctors and agronomists who have great concerns. Many associations are denouncing these dangers. Many others, grouping together, such as farmers wish to exercise their profession outside of the facilities offered by chemical products. In the same chain of thought, everyone knows that the food businesses, supposedly called “dietetic” or “weight losing” regimes, have an increasing success when they attach themselves more and more to the idea of securing or buying foods prepared without artifice, without adulteration, excepting the help of nature only.
None of this is a mystery. It becomes more and more popular.
My work’s aim is this subject. It has always been the object of many studies in the La Presse as well as in diverse writings. I am pleased to say here that the certitude of the progression of evil, physical and moral decrepitude, towards which we tend, does not come strictly from the causes mentioned. It comes from the non-observance of the law, of which I speak, at the beginning of this introduction. Awareness of this law is already a step able to help turn events. I will try to reach you, more, with my letters, following: I have destined them for you.
Full Work Here Reprinted without permission as email address now invalid.
Walnuts are rich in omega-3 fatty acids, phytochemicals and antioxidants making them unique compared to other foods. Consuming walnuts has been associated with health benefits including a reduced risk of heart disease and cancer. Dysbiosis of the gutmicrobiome has been linked to several chronic diseases. One potential mechanism by which walnuts may exert their health benefit is through modifying the gut microbiome.
This study identified the changes in the gut microbial communities that occur following the inclusion of walnuts in the diet.
The diet groups had distinct microbial communities with animals consuming walnuts displaying significantly greater species diversity. Walnuts increased the abundance of Firmicutes and reduced the abundance of Bacteriodetes.
Glycemic load chart below should be used as a guide to make wiser food choices to perform better all day long and feel better generally by keeping your blood glucose levels relatively constant.
If there is a sudden spike in your blood sugar, your pancreas secretes more insulin, bringing your blood sugar down by transforming the excess sugar to fat. The higher the rate is, the lower your blood sugar will go. Blood glucose being too low means increased hunger and fatigue.
Glycemic index and glycemic load are both about the impact of carbohydrate rich foods on your blood glucose levels or in other words how quick or slow they cause a rise and a fall.
The difference is that glyemic load is based on the idea that a small serving of a high GI food will have the same kind of effect as a big serving of a low GI food. Foods that are mostly water, for instance, will not cause a sudden rise in your blood sugar even if they have high GI values.
That’s how they’ve come up with the glycemic load- GL. GL takes into account both the GI value and the quantity of carbohydrate in that food. So it provides a more accurate picture than glycemic index, as you will see on the glycemic load chart below.
Glycemic Load = (Quantity of carbohydrate content x GI ) / 100.
• GL of 20 or more is high, a GL of 11 to 19 is medium and a GL of 10 or less is low.
• A food with a GI of 70 and a carb content of 10g has a GL value of 7.
• A food with a GI of 10 and a carb content of 70g has also a GL value of 7.
Glycemic Load Chart:
Dairy Products:
• Full cream milk — 250ml — 3
• Soy milk — 250ml — 4
• Skimmed milk 250ml — 4
• Semi skimmed milk — 250ml — 4
• Low fat ice cream — 50g — 6
• Low fat fruit yogurt — 200g — 7
• Banana smoothie — 250ml — 8
• Mars flavoured milk — 250ml — 15
Fruits:
• Grapefruit — 120g — 3
• Cherries — 120g — 3
• Peach — 120g — 4
• Watermelon —120g — 4
• Pear — 120g — 5
• Plum — 120g — 5
• Orange — 120g — 5
• Apricot — 120g — 5
• Apple — 120g — 6
• Grapes — 120g — 8
• Banana — 120g — 12
• Sultanas — 60g — 25
• Raisins — 60g — 28
Vegetables:
• Broccoli — 80g — 1
• Cabbage — 80g — 1
• Spinach — 80g — 1
• Asparagus — 80g — 1
• Carrot — 80g — 3
• Green peas — 80g — 3
• Broad beans — 80g — 9
• Parsnips — 80g — 12
• Sweet potato — 150g — 17
• Sweet corn — 150g — 17
• Baked potatoes — 150g — 26
Legumes:
• Soy beans — 150g — 1
• Lentils — 150g — 5
• Split peas — 150g — 6
• Baked beans — 150g — 7
• Red kidney beans — 150g — 7
• Garbanzos — 150g — 8
• Romano beans — 150g — 8
• Pinto beans — 150g — 10
• Navy beans — 150g — 12
Grains:
• Barley — 150g — 11
• Bulgur — 150g — 12
• Whole wheat kernels — 50g — 14
• Brown rice — 150g — 18
• Couscous — 150g — 23
• White rice — 150g — 23
Cereals:
• Muesli — 30g — 10
• Porridge — 250g — 12
• Kellogg’s All Bran — 30g — 12
• Swiss muesli — 30g — 13
• Oatmeal — 250g — 13
• Kellogg’s Special K — 30g — 14
• Puffed wheat — 30g — 16
• Instant oatmeal — 250g — 17
• Corn flakes — 30g — 19
• Coco pops — 30g — 20
Breads:
• Burgen fruit loaf — 30g — 6
• Pumpernickel Bread — 30g — 6
• Barley and sunflower bread — 30g — 6
• Rye bread — 30g — 7
• Rice bread — 30g — 8
• Whole wheat bread — 30g — 9
• White pita bread — 30g — 10
• Baguette — 30g — 10
• White bagel — 30g — 11
Snacks and Beverages:
• Tomato juice — 250ml — 2
• Apple juice — 250ml — 10
• Carrot juice — 250ml — 10
• Banana cake — 80g — 12
• Vanilla wafers — 25g — 14
• Corn tortilla — 60g — 14
• Pepsi — 250ml — 15
• Cranberry juice drink — 250ml — 16
• Sponge cake — 60g — 16
• Rice cakes — 25g — 17
• Snickers bar — 60g — 19
• Fanta — 250ml — 23
*Foods with low GL values are almost always low in glycemic index too. Those with medium or high GL could be anything- from very low to very high GI.
*You can only see the glycemic load values of foods on the Glycemic Load Chart above, if you would like the glycemic index values as well, please refer to the Glycemic Index Chart, where you can make a comparison between glycemic index and glycemic load values of carbohydrate rich foods.
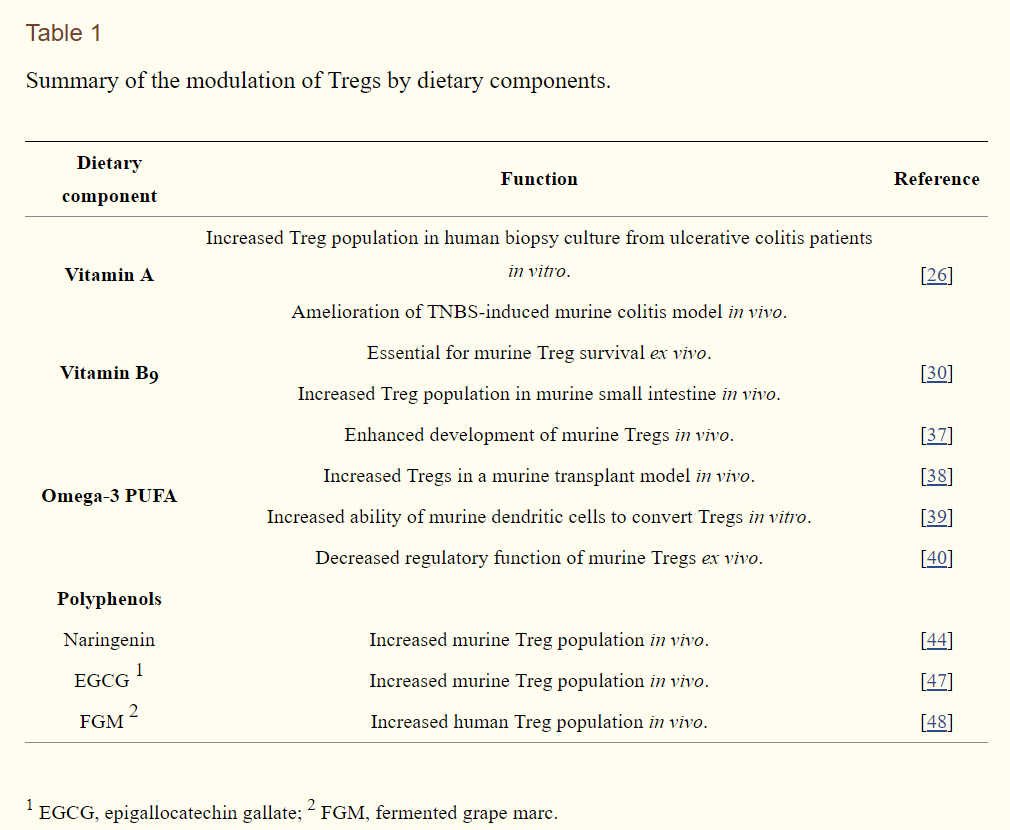
Many clinical and animal studies have shown that certain dietary components exert anti-inflammatory properties that aid in the amelioration of chronic inflammatory diseases. Among the various proposed channels through which dietary components affect immune responses, regulatory T-cells (Tregs) are emerging as key targets for the dietary prevention of chronic inflammatory diseases. In this review, immunoregulation by Tregs is briefly described, followed by a summary of recent advances and possible applications of techniques for the study of Tregs. In addition, this review provides an overview of the current knowledge on Treg regulation by certain dietary components, including vitamins, omega-3 polyunsaturated fatty acids, and polyphenols. The caveats of previous studies are also discussed in order to highlight the distinctions between dietary studies and immunological approaches. Consequently, this review may help to clarify the means by which nutritional components influence Tregs.
Following dietary consumption and absorption in the intestines, water-insoluble vitamin A (all-trans-retinol) is carried by cellular retinol binding protein (CRBP) in an aqueous environment to be transported into the cytoplasm. Subsequently, retinol is oxidized to retinal by retinol dehydrogenase, and then retinal is further oxidized to retinoic acid by retinal dehydrogenase [25]. With respect to the role of vitamin A in the development of Tregs, Bai et al. [26] demonstrated that the population of Tregs derived from biopsies of ulcerative colitis patients increases following ex vivo culture in the presence of retinoic acid, a potent metabolite of vitamin A. In the same study, using a chemical (2,4,6-trinitrobenzene sulfonic acid, TNBS)-induced murine colitis model, it was further elucidated that dietary vitamin A ameliorated colitis, which is accompanied by an increased population of Tregs. Wu et al. [27] further reported that intraperitoneal administration of all-trans retinoic acid aided in the attenuation of airway inflammation by inducing Treg development in a model of experimental allergic asthma. Moreover, a dietary study demonstrated that retinal intervention in mice upregulated Tregs, which further assisted in the treatment of autoimmune inflammatory disorders, including rheumatoid arthritis [28]. Overall, these animal studies indicate that vitamin A and its metabolites affect populations of Tregs, thereby suppressing chronic inflammatory diseases. However, it remains unclear whether vitamin A affects Tregs directly, indirectly, or both. Indeed, Chang et al. demonstrated that dendritic cells also promote the generation of Tregs in response to retinoic acid, at least in vitro [29], exemplifying that in vivo models are more complicated for elucidating the mechanism of action of dietary components.
With respect to water-soluble vitamins, Kunisawa et al. [30] showed that Tregs express high levels of vitamin B9 (folic acid) receptor on their cell surfaces. Furthermore, vitamin B9 was demonstrated to be a survival factor for Tregs; in a vitamin B9-deficient culture, naïve CD4+ T-cells successfully differentiated into Foxp3+ Tregs but failed to survive. Moreover, it was found that mice fed a vitamin B9-deficient diet exhibited a decreased number of Tregs in the small intestine, where vitamin B9 is absorbed.
4.2. Dietary Fatty Acids
A significant quantity of data has indicated that dietary omega-3 polyunsaturated fatty acids (PUFA) may prevent or ameliorate chronic inflammatory diseases, including inflammatory bowel diseases [31,32,33,34]. These studies have identified multiple anti-inflammatory mechanisms of omega-3 PUFA: cytokine production, antagonism to omega-6 PUFA metabolism, binding to nuclear receptors as ligands, the alteration of signaling protein acylation, and the modulation of signaling platform lipid rafts in various immune cell models. With respect to CD4+ T-cell mediated inflammatory responses, several studies using dietary intervention with either purified omega-3 PUFA or fish oil (which is rich in omega-3 PUFA) demonstrated that CD4+ T-cell functions, as assessed by cytokine production and proliferation, were suppressed in both humans [35,36,37] and experimental animals [38,39].
As for the effect of omega-3 PUFA on Tregs, it was shown that the omega-3 PUFA abundant in fermented fish oil enhanced the development of Foxp3+ Tregs in vivo [40]. Moreover, intraperitoneal injection of eicosapentaenoic acid (EPA), an omega-3 PUFA, resulted in prolongation of graft survival in a murine transplant model, accompanied by an increased population of Tregs [41]. However, those studies do not conclusively demonstrate a direct function of omega-3 PUFA on the differentiation and/or function of Tregs, given the caveat that in vivo administration of omega-3 PUFA can affect diverse types of accessory cells. Indeed, it was found that dendritic cells cultured in docosahexaenoic acid (DHA, an omega-3 PUFA)-rich conditions facilitated the development of Tregs, at least in vitro [42], indicating an indirect modulation of Treg development by omega-3 PUFA. However, despite the increase in the development of Tregs, the favorable effect of omega-3 PUFA on Tregs is still controversial because it has also been observed that DHA inhibited the suppressive effect of Tregs on effector T-cell proliferations in a dose-dependent manner in vitro [43].
4.3. Dietary Polyphenols
Dietary polyphenols are well known for their antioxidant properties, which can further suppress inflammatory responses by reducing nitric oxide. In addition to their archetypal antioxidant capacities, immunoregulatory effects of select polyphenols on Tregs have been characterized as follows. Wang et al. [44] reported that ex vivo development of CD4+ Foxp3+ Tregs was induced in the presence of the flavonoid naringenin in part via activation of the aryl hydrocarbon receptor, a transcription factor. As well, increased Treg differentiation suppressed the proliferation of effector T-cells. In addition, dietary naringenin was found to suppress cholesterol-induced systemic inflammation, metabolic dysregulation, atherosclerosis, and allergen-induced airway inflammation [45,46], although it was not clear whether those inhibitory effects were Treg-dependent. In a mouse model of T-cell mediated inflammatory disease of the central nervous system, dietary intake of epigallocatechin gallate (EGCG), a catechin derivative, exerted a favorable effect, in part by increasing the Treg population in the spinal cord [47]. Furthermore, fermented grape marc (FGM) was found to promote Treg differentiation of human CD4+ T-cells [48].Go to:
5. Conclusions
Due to the relatively short history of studies on Tregs, investigations of the direct effects of a variety of dietary components on Treg conversion are limited at present (summarized in Table 1 and previously reviewed elsewhere [49]). It seems that a majority of the anti-inflammatory functional studies have been conducted in vivo by observing physiological outcomes, such as symptoms of chronic inflammation and accumulation of certain immune cell types. Even though in vivo studies are indispensable for nutritional studies, simpler model systems must be developed to dissect the detailed mechanisms by which dietary components regulate physiological systems. Therefore, further studies using more sophisticated and appropriate in vivo model systems are needed to draw solid conclusions. In this regard, as introduced in this review, the protocol for Treg differentiation from naïve CD4+ T cells could be effectively utilized to determine the direct effects of a variety of promising dietary Treg modulators present in foods.