David Carr, M.D., from University of California in San Diego, and H. Gilbert Welch, M.D., a general internist in Thetford, Vermont, used the Open Payments database to determine industry payments made to physician directors of NCI-designated cancer centers (2015 through 2017).
The researchers found that of the 53 physician cancer center directors listed in 2017, 44 held the position in 2016 and 41 in 2015. In 2017, payments totaled $4.42 million, including $1.89 million in research payments to 12 directors and $2.53 million in nonresearch payments to 22 directors. Half of directors (51 percent) received no payments, while more than one-third (36 percent) received more than $5,000. Physician directors were more likely to receive payments unrelated to research than they were to receive research payments, with 12 of the 53 directors receiving payments unrelated to research exceeding the $5,000 threshold (defined as a significant financial interest by the NCI) and two receiving payments of more than $50,000. In 2017, 12 directors received research payments, with four receiving more than $50,000.
“Our findings raise the question of whether industry payments to the directors of publicly supported institutions, such as NCI-designated cancer centers, serve the public interest,” the authors write.
The effects of calcium ion and broad pH ranges on free fluoride ion aqueous concentrations were measured directly and computed theoretically.
Solubility calculations indicate that blood fluoride concentrations that occur in lethal poisonings would decrease calcium below prevailing levels.
Acute lethal poisoning and also many of the chronic effects of fluoride involve alterations in the chemical activity of calcium by the fluoride ion.
Natural calcium fluoride with low solubility and toxicity from ingestion is distinct from fully soluble toxic industrial fluorides.
The toxicity of fluoride is determined by environmental conditions and the positive cations present. At a pH typical of gastric juice, fluoride is largely protonated as hydrofluoric acid HF.
Industrial fluoride ingested from treated water enters saliva at levels too low to affect dental caries.
Blood levels during lifelong consumption can harm heart, bone, brain, and even developing teeth enamel.
The widespread policy known as water fluoridation is discussed in light of these findings.
Full = https://www.hindawi.com/journals/jeph/2013/439490/
A burgeoning body of research confirms and affirms the presence of aluminium in human brain tissue. Recently, the first data on aluminium content of brain tissue from donors with diagnoses of familial Alzheimer’s disease, autism spectrum disorder, multiple sclerosis and epilepsy have been published. Quantitative data are supported by aluminium-specific fluorescence microscopy identifying the locations of aluminium in human brain tissue.
The challenge in the future will be to confirm or refute the role played by brain aluminium intoxication in human neurodegenerative disease.
Human exposure to aluminium is burgeoning [1]. Living in the ‘aluminium age’ ensures that the myriad ways in which we are exposed to aluminium today will be even more numerous tomorrow. Aluminium in human brain tissue is the inevitable consequence of this burgeoning exposure [2]. However, what are the consequences of aluminium in human brain tissue? We know that aluminium does not benefit the human brain and in ‘excessive amounts’ it is neurotoxic. The latter label of ‘neurotoxicity’ is widely accepted for humans only because of the experience of relatively rare occurrences of iatrogenic disease [3] and especially dialysis dementia [4]. While aluminium in brain tissue is inevitable when is it also toxic? How can we define toxicity thresholds and when does neurotoxicity achieve a phenotype in affected individuals. How much aluminium in brain tissue is too much?
We reviewed aluminium in human brain tissue almost 10 years ago [2] and in the period since, out with research in our group, there have not been any new quantitative data published on this subject. In 2012, we published the results of our 60 human brain study, an undertaking designed to provide robust and unequivocal data on the aluminium content of human brain tissue [5]. The research applied the most rigorous quality assurance methods possible including the measurement of 174 method blanks. We defined a method blank as an estimate of sample contamination from all experimental procedures beginning with taking tissue samples at the brain bank through to analyses of brain digests by transversely heated graphite furnace atomic absorption spectrometry (TH GFAAS). The only difference with sample treatments being that method blanks did not include brain (any) tissues. The median amount of aluminium present as a contaminant was 22 ng/reaction vessel (used for microwave-assisted digestion) and since the method blank data were not normally distributed, a log transformation was used to determine a contaminant level of 54 ng/reaction vessel (mean + 1.654SD). This value is, thereafter, subtracted from all tissue digests carried out using identical experimental procedures. The final data obtained for 60 human brains were revealing in a number of ways. In the first instance, the median aluminium content for all 713 tissue samples was 1.02 μg/g dry wt., an aluminium content in human brain tissue that might be thought of as inevitable (in donors aged 70–103 years) if not normal. However, scrutiny of data showed that in 41 of the 60 donors, the aluminium content of at least one tissue was above 3.00 μg/g dry wt., an aluminium content thereafter defined as pathologically significant [6]. While the brain bank that provided these tissues refused (retrospectively) to reveal the disease state of the individual donors it is a matter of published record that for this particular brain bank approximately 50% of donors had a diagnosis of dementia at death [7]. As such, the 60 human brain data set for aluminium constituted about 30 donors with a diagnosis of Alzheimer’s disease and 30 aged controls.
The nature of the aluminium data for the 60 human brains, range 0.01–33.00 μg/g dry wt., confirmed that which was already suspected, the focal as opposed to homogenous distribution of aluminium in human brain tissue [8]. It also questioned the value of brain tissue data based solely upon averages. Mean or median values would be informative where tissues were heavily overloaded with aluminium, but generally these statistics are more likely to hide important data on focal accumulations of aluminium. For example, not revealing areas of the brain where the aluminium content is sufficiently high to bring about, at the very least, focal neuropathology. We published the aluminium content of each of the three replicates of each tissue and eschewed the calculation of averages. We have continued the practice of publishing data for all replicates in all subsequent studies on aluminium in human brain tissue.
It is a rare privilege to work with human brain tissue, and weights of tissues available through brain banks are usually limited to less than 1 g. However, on some occasions, an opportunity arises to analyse larger weights of tissue and we had such an opportunity for a case of Alzheimer’s disease linked to occupational exposure to aluminium [9]. We were provided with approximately 20 g frozen weight of the frontal lobe and this was divided into approximately 50 separate samples. Our 60-brain study had identified 0.3–0.5 g as the optimal range for fresh weight of brain tissue. Wet weights below 0.3 g could result in dry weights where the influence of contaminating aluminium might be disproportionately high, whereas wet weights above 0.5 g were prone to incomplete digestion in the microwave. The concentration of aluminium (mean and SD) in the frontal lobe of brain tissue from this occupationally exposed individual was 2.98 (2.73) μg/g dry wt. for 46 replicates. That 35% of the replicates had a concentration of aluminium above 3.00 μg/g dry wt. confirmed a possible role for aluminium in this individual’s early-onset Alzheimer’s disease. Once again, as was the case for brain tissues in the 60-brain study, the range of concentrations was wide from the limit of detection, 0.01–12.97 μg/g dry wt. and demonstrated the focal distribution of aluminium in human brain tissue.
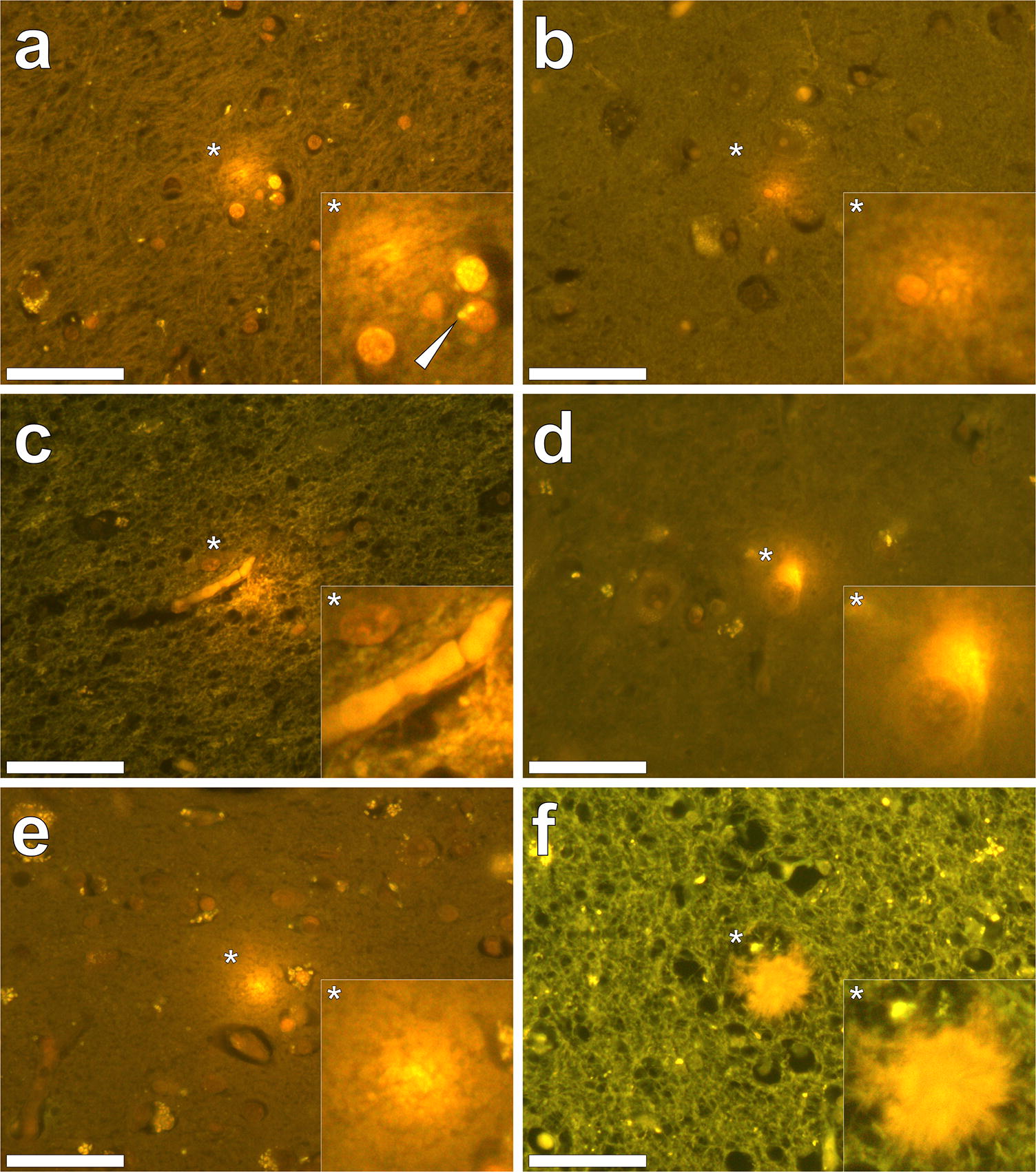
Our subsequent studies have measured the aluminium content of brain tissue from donors who died with a diagnosis of familial Alzheimer’s disease (fAD) [10], autism spectrum disorder (ASD) [11], multiple sclerosis (MS) [12] and epilepsy [13]. In fAD the concentration of aluminium ranged from 0.01 to 35.65 μg/g dry wt. with 11 out of 12 donor brains having at least one tissue where the aluminium content is considered as pathologically significant (≥ 3.00 μg/g dry wt.). For ASD the concentration of aluminium ranged from 0.01 to 22.11 μg/g dry wt. with five out of five donor brains having at least one tissue where the aluminium content was considered as pathologically significant (≥ 3.00 μg/g dry wt.). In MS donor tissue, aluminium concentrations ranged from 0.01 to > 50 μg/g dry wt. and all 14 donors had at least one tissue where the aluminium concentration was considered pathologically significant (≥ 3.00 μg/g dry wt.). Peer review of these published studies has consistently asked how brain aluminium data compare with control donor brains. In addressing this important criticism, a pertinent question is what constitutes control tissue in brain aluminium research. For example, is brain tissue from a donor who has not died from a particular disease, e.g. MS, suitable control tissue for that condition? It should be recognised that aluminium is a toxin and its presence in brain tissue is only inimical. All biologically reactive aluminium will be disruptive and, at the very least, will require energy use in compensating its presence. At some point, compensating a toxic threshold of aluminium will manifest as neurodegeneration identifiable as such by an experienced pathologist. Brain banks are not replete with healthy brains. The majority of brains are from aged donors with underlying conditions. To understand the role of aluminium in neurodegenerative disease including AD, ASD and MS, age- and gender-matched healthy control brains are required. If available, such brain tissues would help in understanding if high concentrations of aluminium contribute towards neurodegeneration, for example, high levels of aluminium with no coincident neurodegeneration would suggest otherwise. Similarly, data on healthy brain tissue would help to identify concentrations of aluminium that would not be expected to contribute towards neurodegeneration. We have worked with a major brain bank in the UK to identify donor brains in which there is little or no neurodegeneration. We have identified 21 brains, the majority from aged donors, and we are currently measuring their aluminium content to help to address the points raised above about what constitutes control brain tissue and what content of aluminium we might expect to find in brain tissue unaffected by overt neurodegenerative disease.Quantitative measurements of brain aluminium are informative, but their interpretation with respect of neurotoxicity requires additional information. Previous research has suggested that the distribution of aluminium in brain tissue is focal, being, for example, associated with neuropathology [2]. The recent development of aluminium-specific fluorescence microscopy [14] has not only been helpful in confirming the presence of aluminium in human brain tissue, but it has also identified the location of aluminium (Fig. 1). Imaging of aluminium has put quantitative data in context, for example, while both fAD and ASD showed some of the highest aluminium content, imaging identified clear differences in the location of aluminium. While in fAD deposits of aluminium were primarily extracellular [10], in ASD aluminium was mainly intracellular and associated with non-neuronal cells such as microglia [11]. Imaging has also helped in identifying associations between aluminium and disease-specific neuropathology. For example, in fAD aluminium was co-localised with amyloid in senile plaques [10], whereas in cerebral amyloid angiopathy (CAA) deposits of aluminium were distinct from those of amyloid [15]. Similarly, while aluminium has been linked historically with neurofibrillary tangles in Alzheimer’s disease [16], tau and aluminium were not co-located in late-onset adult epilepsy [13]. In MS, imaging has identified aluminium in both extra- and intracellular locations as well as associated with neuropathology including plaque-like structures and corpora amylacea [12].
Fig. 1Aluminium imaged in the human brain. Lumogallion staining (1 mM in 50 mM PIPES, pH 7.4, 45 min.) of 5 μm brain tissue sections from donors diagnosed with (a–c) autism spectrum disorder (ASD), d cerebral amyloid angiopathy (CAA), e epilepsy and f familial Alzheimer’s disease (fAD). Intracellular aluminium in astrocytes (a, white arrow), microglia b and in endothelial cells in the lumen of a blood vessel c in donors diagnosed with ASD in a white matter of the hippocampus b the frontal cortex and c white matter of the parietal lobe. Intracellular aluminium in a neuronal cell in a donor diagnosed with CAA in grey matter of the hippocampus (d). Extracellular aluminium in the temporal cortex of a donor diagnosed with epilepsy (e) and (f) co-localised with a senile plaque in white matter of the frontal lobe of a donor diagnosed with fAD. Magnified inserts are denoted with asterisks and images were acquired using an Olympus U-MNIB3 fluorescence filter cube (excitation: 470–495 nm, dichromatic mirror: 505 nm, longpass emission: 510 nm). Magnification ×400, scale bars: 50 μm
Aluminium-specific fluorescence microscopy has confirmed that aluminium is not distributed homogenously in brain tissue and this informs us that even when an aluminium concentration of 1.00 μg/g dry wt. (1 ppm) is determined for 0.500 g fresh weight of tissue, there will be regions within this sample of tissue where the concentration of aluminium is significantly higher than 1 ppm. These total concentrations of aluminium will be sources of biologically reactive aluminium with the potential for toxicity and even cytotoxicity [6]. Local toxicity may result in cellular and neuronal dysfunction and evoke compensatory mechanisms in affected cell populations. Where the concentration of aluminium in 0.500 g of fresh weight of tissue is in excess of 3.00 μg/g dry wt., there will be focal concentrations of aluminium in excess of 10 ppm and the consequent local toxicity will be more overt and compensatory mechanisms less effective. Neurotoxicity is inevitable under such conditions and aluminium will either initiate a disease process or accelerate any disease processes that may be ongoing [17].
The presence of aluminium in brain tissue is an intoxication. It will inevitably exert toxicity at a local level. Future research is required to ascertain the significance of discrete aluminium-related neurotoxicity and how the additive effects of such neuropathologies may eventually contribute towards recognised global neurodegenerative disease characteristic of conditions such as AD, MS, epilepsy and ASD.
Sheylla M. Felau, Lucas P. Sales, […], and Fabiana B. Benatti
Abstract
Endothelial cells are thought to play a central role in the pathogenesis of antiphospholipid syndrome (APS). Omega-3 polyunsaturated fatty acid (n-3 PUFA) supplementation has been shown to improve endothelial function in a number of diseases; thus, it could be of high clinical relevance in APS. The aim of this study was to evaluate the efficacy of n-3 PUFA supplementation on endothelial function (primary outcome) of patients with primary APS (PAPS). A 16-week randomized clinical trial was conducted with 22 adult women with PAPS. Patients were randomly assigned (1:1) to receive placebo (PL, n = 11) or n-3 PUFA (ω-3, n = 11) supplementation. Before (pre) and after (post) 16 weeks of the intervention, patients were assessed for endothelial function (peripheral artery tonometry) (primary outcome). Patients were also assessed for systemic markers of endothelial cell activation, inflammatory markers, dietary intake, international normalized ratio (INR), and adverse effects. At post, ω-3 group presented significant increases in endothelial function estimates reactive hyperemia index (RHI) and logarithmic transformation of RHI (LnRHI) when compared with PL (+13 vs. −12%, p = 0.06, ES = 0.9; and +23 vs. −22%, p = 0.02, ES = 1.0). No changes were observed for e-selectin, vascular adhesion molecule-1, and fibrinogen levels (p > 0.05). In addition, ω-3 group showed decreased circulating levels of interleukin-10 (−4 vs. +45%, p = 0.04, ES = −0.9) and tumor necrosis factor (−13 vs. +0.3%, p = 0.04, ES = −0.95) and a tendency toward a lower intercellular adhesion molecule-1 response (+3 vs. +48%, p = 0.1, ES = −0.7) at post when compared with PL. No changes in dietary intake, INR, or self-reported adverse effects were observed. In conclusion, 16 weeks of n-3 PUFA supplementation improved endothelial function in patients with well-controlled PAPS. These results support a role of n-3 PUFA supplementation as an adjuvant therapy in APS. Registered at http://ClinicalTrials.gov as NCT01956188.
The metabolism of (−)-quinate and shikimate by one heterofermentative strain,Łactobacillus pastorianus, and by one homofermentative strain,Lactobacillus plantarum, has been studied using growing and washed cells. Both organisms reduced quinate and shikimate under anaerobic conditions in the presence of suitable hydrogen donors including fructose, glucose andd(−) andl(+)-lactates. The end-product ofL.pastorianus metabolism was dihydroshikimate butL.plantarum carried the reduction a stage further tocis-3,4-dihydroxycyclohexanecarboxylate and formed, simultaneously, catechol. The enzymes involved in these reductions are induced; their importance in the metabolism of lactobacilli is discussed.
ChooseLife Notes : This very old research shows the utter importance of the Shikimate pathway, in Bacterial mutation into crucial life supporting matter.
Recent studies have shown that Omega3 + Lactobacillas plantarum, together down regulate H.pylori 96%
This is a profound reason, in the authors opinion, to avoid Glyphosate (which acts by damaging the Shikimate pathway in environmental bacteria, wonder what eating crops with Glyphosate residue on/in May do to the hosts Bacterial fauna?)
Research compared effects of fresh and thermally processed oil
Date : August 23, 2019
Source : University of Massachusetts at Amherst
Summary : Food scientists have shown that feeding frying oil to mice exaggerated colonic inflammation, enhanced tumor growth and worsened gut leakage, spreading bacteria or toxic bacterial products into the bloodstream.
Foods fried in vegetable oil are popular worldwide, but research about the health effects of this cooking technique has been largely inconclusive and focused on healthy people. For the first time, UMass Amherst food scientists set out to examine the impact of frying oil consumption on inflammatory bowel disease (IBD) and colon cancer, using animal models.
In their paper published Aug. 23 in Cancer Prevention Research, lead author and Ph.D. student Jianan Zhang, associate professor Guodong Zhang, and professor and department head Eric Decker showed that feeding frying oil to mice exaggerated colonic inflammation, enhanced tumor growth and worsened gut leakage, spreading bacteria or toxic bacterial products into the bloodstream.
“People with colonic inflammation or colon cancer should be aware of this research,” says Jianan Zhang.
Guodong Zhang, whose food science lab focuses on the discovery of new cellular targets in the treatment of colon cancer and how to reduce the risks of IBD, stresses that “it’s not our message that frying oil can cause cancer.”
Rather, the new research suggests that eating fried foods may exacerbate and advance conditions of the colon. “In the United States, many people have these diseases, but many of them may still eat fast food and fried food,” says Guodong Zhang. “If somebody has IBD or colon cancer and they eat this kind of food, there is a chance it will make the diseases more aggressive.”
For their experiments, the researchers used a real-world sample of canola oil, in which falafel had been cooked at 325 F in a standard commercial fryer at an eatery in Amherst, Massachusetts. “Canola oil is used widely in America for frying,” Jianan Zhang says.
Decker, an expert in lipid chemistry performed the analysis of the oil, which undergoes an array of chemical reactions during the frying process. He characterized the fatty acid profiles, the level of free fatty acids and the status of oxidation.
A combination of the frying oil and fresh oil was added to the powder diet of one group of mice. The control group was fed the powder diet with only fresh oil mixed in. “We tried to mimic the human being’s diet,” Guodong Zhang says.
Supported by grants from the U.S. Department of Agriculture, the researchers looked at the effects of the diets on colonic inflammation, colon tumor growth and gut leakage, finding that the frying oil diet worsened all the conditions. “The tumors doubled in size from the control group to the study group,” Guodong Zhang says.
To test their hypothesis that the oxidation of polyunsaturated fatty acids, which occurs when the oil is heated, is instrumental in the inflammatory effects, the researchers isolated polar compounds from the frying oil and fed them to the mice. The results were “very similar” to those from the experiment in which the mice were fed frying oil, suggesting that the polar compounds mediated the inflammatory effects.
While more research is needed, the researchers hope a better understanding of the health impacts of frying oil will lead to dietary guidelines and public health policies.
“For individuals with or prone to inflammatory bowel disease,” Guodong Zhang says, “it’s probably a good idea to eat less fried food.”
Aug. 28 (UPI) — People with gout have nearly a 30 percent higher risk of developing chronic kidney disease than people without gout, a new study says.
In addition, those with gout who receive dialysis or need a kidney transplant have more than a 200 percent higher chance of kidney failure than those without gout, according to research published Wednesday in BMJ Open.
Gout is inflammatory arthritis that causes uric acid to build up in the joints, often leading to extreme pain and even debilitation for some.
“While we always believed that high levels of uric acid might be bad for kidneys and that patients with gout may have a higher risk of kidney failure, we were quite surprised by the magnitude of the risk imposed by gout in these patients,” study author Austin Stack, a researcher at University of Limerick in Ireland, said in a news release. “We were particularly interested in the risk of advanced kidney disease, as these patients in general have a higher risk of kidney failure and death.”
The researchers looked at data for nearly 69,000 gout patients from another UK-based study to assess their risk of advanced chronic kidney disease. They compared that data to 554,964 patients without gout.
Diabetes, eating a lot of seafood and meat, drinking alcohol and obesity are all risk factors for gout, according to the Mayo Clinic.
“The result of this new research suggests that gout may also play an important role in the progression of kidney disease,” Stack said. “The identification of gout as a potential risk factor opens up new opportunities for the prevention of kidney disease and its consequences.
Why is it, that many modern diseases of high prevalence, affect some people and not others?
Well? It can’t be the Mercury, they said, as otherwise everyone would get it.
Well? It can’t be the Fluoride, our body needs and produces that.
Well? It can’t be the Aluminium, it’s prevalence means we have historical digestive capability to cope they say, it is such tiny amounts given medically they say.
Well? It can’t be poor diet, the body has homeostasis to set right such problems.
Until we start to look at life from another perspective, illness may hurtle towards us, regularly, with ever more velocity. Given the continual decline in soil quality, producing less vital fruits, vegetables, meats, nuts and seeds (even herbs). The problem is exacerbated by the emergence of processed sugars and flours, which in most guises are antagonistic to our biochemistry, chiefly Calcium (Magnesium, Iodine et al.), which might make a simple walk in the park dangerous, simply a cut or graze might cause an infection.
When fluids in the endosome become too acidic, the cargo is trapped within the endosome deep inside the cell. When the endosome contents are more alkaline, the cargo lingers at the cell’s surface for too long.
They found that mouse cell lines containing the Alzheimer’s disease gene variant had more acidic endosomes (average of 5.37 pH) than cell lines without the gene variant (average of 6.21 pH).
Pretty compelling picture.
The above research, clearly demonstrate that it is when pH of matter falls (or rises) out of its environmental bounds, matter starts to decay and becomes unable to buffer stronger opposing electromagnetic forces, demonstrated by the papers above showing it is pH dropping which really appears to make Mercury, Aluminium & Fluoride (Excessively) Toxic, even in the ‘low’ amounts suggested as safe by regulatory authorities.
This ticks all the boxes of “why some and not others” with Dental Amalgam, Vaccination related side effects (Aluminium Hydroxide pH 9.5 injected into an individual with a tissue pH in the 5.0-5.5 range is hugely more dangerous than an individual in the safer zone of 6-7 – the author believes this is the propellant of many debilitating diseases, the data presented in this article supports this theory).
So, we have a period eating poorly, high sugars, processed carbs, processed meats/dairy. Any part of this combination, as a core part of diet, to the wrong individual, will make the tissue pH plummet, it is all there in the studies. If individuals live like this, then the smallest of environmental pollutants may become lethal (because we lack the buffer system, which may allow the host sufficient robustness to cope, this is what gives the lymphatic system the traction to cycle these toxins out).
If you raise the pH of your terrain (eat more greens & more Omega 3!), you suddenly become less prone to infection and heavy metals become less toxic to you, it is almost like God was trying to pass a message to humanity through Carey Reams, isn’t it?
Higher Fruit and Vegetables, less meat, 22,000 people studied, raises pH of Urine:
In conclusion, a more alkaline diet, higher fruit and vegetable and lower meat intake were related to more alkaline urine with a magnitude similar to intervention studies
CONCLUSIONS: Low urine pH is significantly associated with abnormal glucose tolerance; therefore, measuring urine pH might prove useful for identifying patients at high risk for diabetes.
Simply testing someones pH, may show clearly whether they have the biological capability, at all, to repel these neurotoxins, could life be so simple? (not that I advocate vaccination at all personally, or any unnecessary exposure to these nasty elements, full stop). However, If I was a worried parent, before deciding on vaccination I would test my childs urine pH, to get an indicator the gravity of danger my child faces.Then if their pH was below 6.0 maybe feed them more greens and good oil for a few weeks, test again, then make a more informed decision. This seems eminently sensible.
ChooseLife : pH balancing is the middle path. Developed from thoughts of Randall David Dew, it is time this great man was set free.
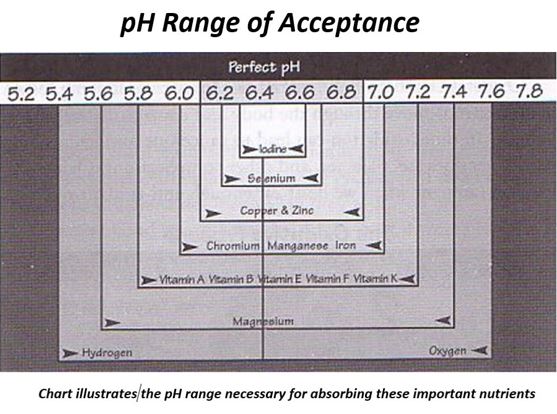
To note, the pH of the ‘high fruit and vegetable diet’, is higher than Carey Reams suggested we should attain, to produce perfect friction (or metabolic energy release between anionic and cationic elements in the body), he suggests 6.4 is perfect urine pH, the same for Saliva pH, which together denote the overall pH terrain status (the mean of 2x Urine 1x Saliva).
As the studies above all show, once your pH is in the range below 5.5 biological function becomes very difficult to sustain, without disease and illness. This dovetails Carey Reams profound teachings about Biological Ionisation, where he demonstrated multiple nutrients cannot be absorbed when the terrain is in this low pH condition (or excessively high also, as shown).