Acidosis is a complex metabolic state with a range of etiologies (Planche and Krishna 2006; Taylor et al. 2012). Within malaria, acidosis is caused by a combination of several factors. The malaria parasite produces Plasmodiumlactate dehydrogenase (pLDH), which creates lactic acid leading to decreased pH. Respiratory distress is a common feature of severe malaria and, through sequestration, somnolence, and/or brain swelling, direct central suppression of the respiratory centers leads to irregular breathing patterns in the setting of acidosis, which may contribute to the pH imbalance. Supportive therapy to protect the airway and more aggressively rebalance the pH may decrease mortality (Cheng and Yansouni 2013).
Background: Macrolide antibiotics are highly active in vitro against B.burgdorferi, but have limited efficacy in the treatment of patients with Lyme Disease. As macrolides are less active at a low pH, their poor clinical activity might be due to localization of borrelia to an acidic endosome, and their activity improved by alkalinization of that compartment with hydroxychloroquine.
Material/methods: 235 patients with a multi-symptom complex typical of chronic Lyme disease, ie fatigue, musculoskeletal pain, and neurocognitive dysfunction and with serologic reactivity against B.burgdorferi were treated with a macrolide antibiotic (eg clarithromycin) and hydroxychloroquine.
Results: Eighty % of patients had self-reported improvement of 50% or more at the end of 3 months. After 2 months of treatment, 20% of patients felt markedly improved (75-100% of normal); after 3 months of treatment, 45% were markedly improved. Improvement frequently did not begin until after several weeks of therapy. There were no differences among the three macrolide antibiotics used. Patients who had been on hydroxychloroquine or macrolide antibiotic alone had experienced little or no improvement. Compared to patients ill for less than 3 years, the onset of improvement was slower, and the failure rate higher in patients who were ill for longer time periods.
Conclusions: These results support the hypothesis that the Lyme borrelia reside in an acidic endosome and that the use of a lysosomotropic agent augments the clinical activity of macrolide antibiotics in the treatment of patients with chronic Lyme Disease. In contrast, the efficacy of tetracycline in such patients is not affected by hydroxychloroquine.
When a younger man, began a journey of researching various healing modalities and happened across Curezone. This was a website which housed various alternative health sub-forums.
After some time perusing the forums, it became clear many were self help groups, yet most lacked the substance of success, verified and repeatable by members.
So, it was with the greatest of elation, that Moreless pH Balancing Forum was found, here there were literally hundreds of ”Success Testimonials”.
This was the foundational basis of this website, as soo very much was learned, from the teachings of Carey Reams and Johanna Budwig, Moreless was a crop consultant based from Reams Biological Farming techniques.
Thank you Moreless.
Moreless :
Hi Ya’ll,
The many Success Testimonials that those have posted as may be seen following this link are because of their own willingness to make the needed changes to help their-self:
And “ANYONE” who chooses to come on this forum or post on any other forum that this Healing Protocol does not work and is Rubbish is basically telling “ALL” of those who have Found Success by applying these Healing Ideas by themself learning to take Personal Responsibility, that you are Crazy and do not know what you are talking about !
It seem to me, that just maybe these folks who choose to Bash these ideas may in fact be the Crazy folks?
For there is “NO” other forum on curezone with as many Success Testimonials, which is not trying to take “YOUR” Hard earned Cash from “YOU” !!!!!!!!!!
Are you among the thousands of people who are struggling with Lyme disease? If you are, you will understand just how painful and debilitating it can be.
According to the Center For Disease Control, there are around 30,000 new Lyme disease cases reported in the U.S each year. However, this is only a small proportion of the 300,000 or so people who are thought to be diagnosed each year. 1
In the UK, the disease is also not unheard of, with around 3,000 cases reported annually.
In Australia, The Lyme Disease Association of Australia estimates that around 300,000 Australians live with the disease.
Since the Australian government refuses to accept that Lyme disease can be contracted in the country, only two weeks of treatment are provided under the Medicare system. This means that many Lyme patients are forced to seek medical treatment overseas at specialist centers such as the Budwig Center here in Spain.
How Do You Get Lyme Disease?
Lyme disease is a tick-borne infectious disease caused by the spirochete bacterium Borrelia Burgdorferi, which is usually transmitted to humans through a tick bite. Mosquitoes, spiders, and mites may also transmit it.
Lyme disease is not contagious, and a person can only be infected if bitten by an infected tick. It is also important to note that ticks do not generally transmit the disease until they have been attached to the host for at least 36 hours.
The most common places that tick bites occur are in forests, woodland, or health areas where you find tick-carrying animals such as deer or mice.
Typically, an incubation period can last from between two days and three and a half months. The bacteria does not always cause disease immediately. It is thought that bacteria can lie dormant and, although present, will not cause any symptoms. However, bacteria still has the potential to cause disease at a later stage.
What Are the Signs and Symptoms?
Those with Lyme disease can exhibit similar symptoms to those with Fibromyalgia and Chronic Fatigue Syndrome in its latter stages.
Although there are thought to be around 100 different Lyme disease symptoms, these can vary widely from person to person. The most common are:-
Erythema Migrans
Flu-like symptoms
Fever or chills
Tiredness
Headaches
Severe fatigue
Circular skin rash (Erythema Migrans)
Aching joints and/or stiff neck
Muscular pain
Disrupted sleep patterns
Memory issues or Brain Fog
In around 70% of cases, patients experience a rash on the skin in the shape of a “bulls-eye.” A large red ring on the outside, with a red circle in the middle. The rash is commonly referred to as Erythema Migrans or an EM Rash.
If left untreated, the infection can spread to the joints, the heart and may even disrupt the central nervous system, peripheral nervous system, and cardiovascular system. In some extreme cases, Lyme disease can result in Pericarditis (Inflammation of external heart tissues) or death from heart blockage.
How Is Lyme Disease Diagnosed?
There are two main tests for diagnosing Lyme disease:
ELISA Test – This is usually the first test carried out and is a type of blood test known as an Enzyme-linked Immunosorbent Assay (ELISA). The ELISA test is used to identify specific antibodies that our bodies produce to fight the Borrelia Burgdorferi bacteria. ELISA testing is not always accurate and, in some cases, can even produce false-positive results caused by other conditions.
Western Blot Test – This form of testing is normally carried out once an ELISA test has been returned as positive. A blood sample is taken, and proteins are split to determine whether there are any antibodies present, used by the body to fight the Borrelia Burgdorferi bacteria.
If both of these tests return as positive, this is usually a clear sign that Lyme disease is the cause. Unfortunately, Lyme testing is not 100% accurate, with many doctors rule out the disease altogether, sometimes without any testing.
At the Budwig Center, we use the Vega test, which is a much better option and has a 93% success rate in identifying Lyme disease.
Judging by what we have heard from our own patients and reports on the internet, a vast number of physicians have somewhat limited knowledge when it comes to diagnosing Lyme disease. We often hear patients being told that the symptoms are related to other conditions such as ME/CFS or Fibromyalgia.
This is probably why the disease is also known as the “great imitator,”â as the symptoms are similar to so many other chronic conditions.
Can you prevent Lyme disease?
There are some tips which can help you to decrease the possibility of catching a tick bite. It is recommended to wear long pants and long-sleeved shirts when you are in forests, woodland, or health areas where you find tick-carrying animals such as deer or mice and use insect repellent. It is also vital that you remain vigilant and check yourself, your children, and your pets for ticks. Some assume that you can’t get infected if you’ve had Lyme disease before; however, this is not the case. If you do notice a tick, remove it with tweezers. It is important to check closely whether all tick parts have been removed.
Effective Natural Treatment of Chronic Lyme Disease
Those treated with antibiotics in the early stages of a Lyme infection usually recover completely and in a relatively short space of time.
Unfortunately, the same cannot be said for around 20% of patients who will continue to experience persistent and recurring symptoms. These patients are classed as having PTLDS or Post Treatment Lyme Disease Syndrome.
Post-Lyme disease syndrome symptoms are similar to the symptoms that occur during the early stages. These symptoms include difficulty sleeping, fatigue, joint and muscle aches, short-term memory issues or difficulty concentrating, pain, and swelling in the larger joints, such as elbows, knees, shoulders, or speech issues. It’s fair to say that Lyme disease is one of the most challenging conditions to recover from fully, especially when at a more advanced stage.
Here at the Budwig Center clinic, our experienced therapists have successfully treated many Lyme disease patients over the last 10 years using BioMagnetism or BIO-MAGNETIC THERAPY.
This therapy consists in a trained therapist strategically placing magnets with the correct potency (1000 gauss strength) on the body of a patient to change the pH of the organs treated. When the pH of said organ is neutral, this makes it inhabitable for cancer cells as well as other microorganisms.
Bacteria and parasites live and grow in an alkaline environment while fungus and viruses live and grow in an acidic environment but neither can live in an environment with a neutral pH (7,4). This pH is obtained by placing a set of magnets with opposing polarities, one positive and the other negative, on the pairs of organs affected by the pathogen.
This therapy is compatible with the Budwig protocol as it is helping a person’s body attain a balanced pH and a stronger immune system without using electricity, chemicals or other invasive methods.
The Biomagnetic Pair Therapy was developed in 1988 by Dr. Isaac Goiz Duran, MD. He is not heard of in the English speaking world because he has spent most of his career and made inroads mainly amongst the Spanish speaking cultures. He treated over 350 000 patients using this therapy and trained more than 20 000 medical doctors and other therapists from many different countries.
Because the root of cancer as well as other chronic illnesses is rooted in an unbalanced pH and the presence of microorganisms, we include this therapy in the program for cancer patients and others needing to recuperate their health.
You simply lie down on a massage type table, fully clothes and the therapists tests where to place the magnets using a kinesiology muscle testing method. Our therapist has been mainly practicing this method of treatment since becoming a therapist so he is very experienced and you will likely find his comments very insightful.
Effective Natural Treatment of Chronic Lyme Disease
Those treated with antibiotics in the early stages of a Lyme infection usually recover completely and in a relatively short space of time.
Unfortunately, the same cannot be said for around 20% of patients who will continue to experience persistent and recurring symptoms. These patients are classed as having PTLDS or Post Treatment Lyme Disease Syndrome.
Post-Lyme disease syndrome symptoms are similar to the symptoms that occur during the early stages. These symptoms include difficulty sleeping, fatigue, joint and muscle aches, short-term memory issues or difficulty concentrating, pain, and swelling in the larger joints, such as elbows, knees, shoulders, or speech issues. It’s fair to say that Lyme disease is one of the most challenging conditions to recover from fully, especially when at a more advanced stage.
Here at the Budwig Center clinic, our experienced therapists have successfully treated many Lyme disease patients over the last 10 years using BioMagnetism or BIO-MAGNETIC THERAPY.
UK based practitioner : https://thesouthdownclinic.co.uk/home/therapies/biomagnetic-pair-therapy/
Chooselife : My dear late friends Don and Carol Croft were the inventors and pioneers of Orgonite, one of their profound inventions was the Orgonite Zapper (Hulda Clark based technology, with Orgonite block added):
(no idea if the above Zapper site is better/worse than an Orgonite based Zapper, as it has been too many years since I mixed in these circles, this website has no affiliation with these or any other sellers, Don and Carols website was www.worldwithoutparasites.com )
Wellcome Trust Centre for Cell-Matrix Research, School of Biological Sciences, Faculty of Biology, Medicine and Health, Manchester Academic Health Sciences Centre, University of Manchester, Manchester M13 9PT, U.K.
Abstract
Mucus plays a vital role in protecting the lungs from environmental factors, but conversely, in muco-obstructive airway disease, mucus becomes pathologic. In its protective role, mucus entraps microbes and particles removing them from the lungs via the co-ordinated beating of motile cilia. This mechanism of lung defence is reliant upon a flowing mucus gel, and the major macromolecular components that determine the rheological properties of mucus are the polymeric mucins, MUC5AC and MUC5B. These large O-linked glycoproteins have direct roles in maintaining lung homeostasis. MUC5B is essential for interaction with the ciliary clearance system and MUC5AC is up-regulated in response to allergic inflammatory challenge. Mucus with abnormal biophysical properties is a feature of muco-obstructive respiratory disease and can result from many different mechanisms including alterations in mucin polymer assembly, mucin concentration and the macromolecular form in mucus, as well as changes in airway surface hydration, pH and ion composition. The abnormal mucus results in defective lung protection via compromised ciliary clearance, leading to infection and inflammation.
Mucus plays a vital role in protecting the lungs from environmental factors, but conversely, in muco-obstructive airway disease, mucus becomes pathologic. In its protective role, mucus entraps microbes and particles removing them from the lungs via the co-ordinated beating of motile cilia.
Authors: Grace Russell,1*Alexander Nenov,2 John T. Hancock1 1. Department of Applied Sciences, University of the West of England, Bristol, UK 2. Water Fuel Engineering, Liquorice Way, Pontefract, UK *Correspondence to Grace2.Russell@live.uwe.ac.uk Disclosure: Dr Nenov is a board member of Water Fuel Engineering. The remaining authors have declared no conflicts of interest. Received: 03.02.21 Accepted: 16.03.21
Abstract
Oxy-hydrogen gas (HHO) is a gaseous mixture of molecular hydrogen and molecular oxygen that is generated by the electrolysis of water and delivered in a 2:1 ratio (66% and 33%, respectively) through the use of noninvasive inhalation devices such as nasal cannulas or nebulisers. Although there is a paucity of scientific evidence supporting this new and emerging therapy, initial investigations indicate that HHO proffers cytoprotective qualities, typically by reducing oxidative stress and attenuating the inflammatory response. These aspects are particularly favourable when considering respiratory medicine because underlying inflammation is known to drive the pathological progress of numerous respiratory conditions, including asthma, chronic obstructive pulmonary disorder, and, pertinently, coronavirus disease (COVID-19). Direct delivery to the lung parenchyma is also likely to increase the effectiveness of this emerging medical therapy.
This narrative review aims to delineate how this particular combination of gases can affect cellular processes at the molecular level by focussing on the evolutionary requirement for both oxygen and hydrogen. Furthermore, the authors assess the current available data for the safety and efficacy of HHO in a clinical setting.
ChooseLife : We have a nebuliser and use it now and again, with 1% or so H2O2, but personally think small sips of Milk of Magnesia (pH 11.5) to coat the throat, bring the pH up and let the body start healing itself is best (the Magnesium is shown to loosen sticky mucous), though I am positive towards this research.
Wenju Lu, Xiaoqing Liu, Tao Wang, Fei Liu, Airu Zhu, and Yongping Lin
Patients with coronavirus disease 2019 (COVID-19) exhibit a spectrum of respiratory symptoms like cough and dyspnea.1–3 Airway mucus is an adhesive viscoelastic gel composed mostly of high-molecular-weight mucous glycoproteins and water, which is important in maintaining lung function and health, pathological mucus hypersecretion may cause airway obstruction and lead to respiratory distress. Mucin (MUC) glycoproteins are the major macromolecular components of mucus, which are classified into two major types: the gel-forming secreted MUC5AC and the membrane-tethered MUC1.4 Here, with an attempt to understand the lung changes, we sought to provide a delineation of the components of airway mucus from patients with COVID-19.
To clean airway obstruction, respiratory tract mucus was aspirated and collected via bronchoscopy from COVID-19 patients with a critical illness, and optical coherence tomography (OCT) was applied via bronchoscopy to obtain cross-sectional images of the bronchiole. For healthy control, sputum was induced by inhaled hypertonic (3%) saline solution delivered with an ultrasonic nebulizer. After collection, sputum was processed as previously described for components analysis.5 Medical history, and clinical and laboratory data of the participants were extracted from electronic medical records. The study was approved by the Ethics Committee of the First Affiliated Hospital of Guangzhou Medical University (No. 2020-65). The requirement for informed consent was waived because the study was observational and the family members were in quarantine.
MUC5AC (sc-21701; Santa Cruz, Shanghai, China) and MUC1 (sc-6827; Santa Cruz) in airway mucus were measured using enzyme-linked immunosorbent assay, and MUC1-cytoplasmic tail (CT, clone EP1024Y; Abcam, Shanghai) levels were measured by Western blot analysis as described previously.5 The levels of MUC5AC and MUC1 were normalized to their average signal reading of a healthy control group.
A total of 16 patients with COVID-19 were included in this study, the clinical characteristics of the recruited subjects were shown in Table S1. There was no significant deviation in the distribution of age, or sex between the cohorts of case and control subjects. All the patients with COVID-19 were admitted to the intensive care unit because of low oxygenation index (199 ± 23 mm Hg), and 79% of them received mechanical ventilation. Blood laboratory tests showed elevated inflammatory indexes including leukocyte count, C-reactive protein, and interleukin-6 in most of the patients with COVID-19 (Table S2).
OCT indicated clear bronchiole in healthy controls (Figure 1A) and mucus retention in the bronchiole of patients with COVID-19 (Figure 1B). A volume of 1-8 mL white to gray sputum with high viscosity (Figure 1C) was aspirated from the respiratory tract of 16 patients with COVID-19. Induced sputum from healthy control was clear and transparent with low viscosity. Compared to healthy control, airway mucus from patients with COVID-19 had a higher level of MUC5AC (Figure 1D), MUC1 (Figure 1E), and MUC1-CT fragment (Figure 1F). However, there were no significant differences in the concentration of total protein, sodium, or chloride in the airway mucus from patients with COVID-19 when compared to healthy control (Table S3).
Representative cross-sectional images of bronchioles in (A) healthy and (B) critical ill COVID-19 patients were obtained with optical coherence tomography and bronchoscopy. C, Airway mucus aspirated by bronchoscopy. D, MUC1 and (E) MUC5AC protein levels as measured by ELISA, and (F) MUC1-CT level as measured by Western blot analysis in the airway mucus from COVID-19 patients and healthy control (HC). The levels of MUC5AC and MUC1 were normalized to their average signal reading of healthy control group. COVID-19, coronavirus disease 2019; CT, cytoplasmic tail; ELISA, enzyme-linked immunosorbent assay; MUC, mucin
Although more than half of patients with COVID-19 presented with a dry cough,6 this study provided direct evidence showing mucus retention in the small airway of patients with COVID-19, and patients were not able to expectorate by themselves and need bronchoscopy aspiration to help them to clean respiratory tract. The sputum from these patients with COVID-19 was viscous, which is not surprising as MUC5AC levels are extremely high, hyperconcentration of this gel-forming MUC dehydrates airway surfaces and causes mucus adhesion, which may contribute to airflow obstruction and respiratory distress. Clearance of airway mucus is an important way to increase oxygen and carbon dioxide exchange, bronchoscopy aspiration of airway mucus was used in all our patients to relieve hypoxia. In our center, all the 16 critical ill COVID-19 patients recovered and were discharged from hospitalization, which may attribute to our aggressive clearance of the respiratory tract. It is of note that bedside bronchoscopy may not be available in some hospitals as the medical resources are limited during the COVID-19 pandemic, carbocisteine has been reported to inhibit airway MUC5AC secretion, which could be used to reduce sputum viscosity and elasticity in patients with COVID-19. In addition, hydration of sputum by aerosolized hypertonic saline solutions or mannitol, and dilation of bronchi via aerosolized salbutamol may facilitate sputum expectoration.
MUC1 is a membrane-tethered MUC expressed on the apical surface of epithelial cells.7, 8 Since MUC1-CT fragment is on the cytoplasmic side of the cells, the elevated sputum CT fragment in patients with COVID-19 could come from detached and disrupted epithelial cells, which is evidenced by the pathological findings of diffuse alveolar damage with fibromyxoid exudates and macrophage infiltration in the lung tissue from patients with COVID-19.9
The limitation of this study is that induced sputum was used in the control group to compare airway mucus aspirated via bronchoscopy from patients with COVID-19, because it was very difficult for the patients with COVID-19 to expectorate sputum even with hypertonic saline solution inhalation.
The findings may suggest that increased level of MUCs in the airway mucus may contribute to the high viscosity of airway mucus and sputum retention in the small airway of patients with COVID-19, airway mucus clearance may be indicated to relieve respiratory distress, and MUC5AC may serve as a target for mucolytic agents in treating COVID-19. And MUC1-CT may serve as an indicator reflecting the severity of airway and alveolar epithelial cell damage.
ACKNOWLEDGMENTS
This study was supported by grants from the National Key R&D Project (2016YFC0903700 and 2016YFC1304102), the National Natural Science Foundation of China (81520108001 and 81770043), and grant specific for COVID-19 study from Guangzhou Institute of Respiratory Health. The authors would like to thank Dr Kwang Chul Kim (University of Arizona) for the invaluable assistance with the manuscript.
CONFLICT OF INTERESTS
The authors declare that there are no conflict of interests.
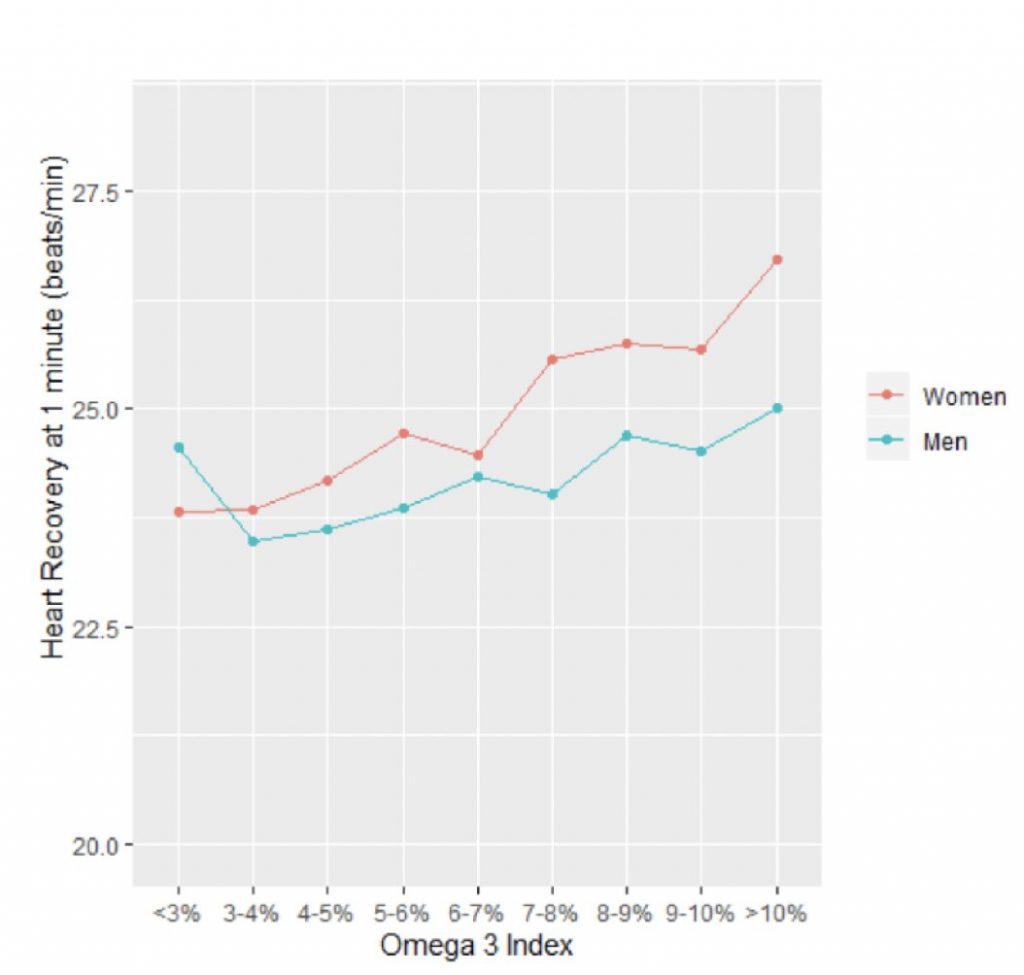
Comparing each patient’s heart rate recovery with their Omega-3 Index, the researchers found a significant relationship between these two variables such that the higher the Index, the faster the heart rate dropped down. The effect was more marked in women than men, but statistically significant in both. This is summarized in Figure 1 (right) where the Omega-3 Index is plotted on the x-axis, and the drop in heart rate one minute after stopping the treadmill test (measured in beats per minute, bpm) is shown as a positive number on the y-axis. Credit: Fatty Acid Research Institute
The Fatty Acid Research Institute (FARI) has published a new research paper in conjunction with The Cooper Institute on omega-3s and heart rate recovery.
Omega-3 fatty acids have a long history of being heart healthy, but exactly why and how has been less clear. They are known to lower serum triglyceride levels, but the effect is relatively small and it’s not clear how much of a risk factor high triglyceride levels is in the first place. So how do the omega-3 fatty acids EPA and DHA work?
A recent study from the Cooper Center Longitudinal Study (CCLS) and FARI sheds new light on this question.
The investigators utilized data from 13,912 healthy men and women who had preventive medical examinations at Cooper Clinic in Dallas over a 10-year period. These examinations routinely included both treadmill exercise testing and measurement of the Omega-3 Index (i.e., red blood cell EPA+DHA levels from OmegaQuant Analytics).
One component of the exercise test is called ‘heart rate recovery’ and it refers to how quickly the heartbeat slows down after maximal exercise. The faster it drops, the healthier the heart.
Comparing each patient’s heart rate recovery with their Omega-3 Index, the researchers found a significant relationship between these two variables such that the higher the Index, the faster the heart rate dropped down. The effect was more marked in women than men, but statistically significant in both. This is summarized in the Figure 1 (right) where the Omega-3 Index is plotted on the x-axis, and the drop in heart rate one minute after stopping the treadmill test (measured in beats per minute, bpm) is shown as a positive number on the y-axis. These are the unadjusted values. (For example, 25 bpm on the y-axis means that 1 minute after stopping exercising—i.e., the maximal heart rate—the person’s heart rate dropped by 25 bpm).
When adjusted for age, maximal METS (a measure of cardiorespiratory fitness), BMI and smoking status, a 2-percentage point higher Omega-3 Index was associated with a 0.35 and 0.69 bpm greater heart rate recovery in men and women, respectively (p<0.001 both).
Previous studies have shown that a slow heart rate recovery is associated with increased risk for sudden cardiac death, which fits with higher EPA and DHA levels being linked with reduced risk for sudden cardiac death3.
Dr. William Harris, President of FARI and co-inventor of the Omega-3 Index, who was also an author on the study, commented on the implications of this research. “These new findings from the CCLS harmonize with the known benefits of omega-3 fatty acids on resting heart rate and provide new clues to how these important fatty acids can preserve cardiac health,” he said.
“These benefits on cardiac autonomic tone join other cardioprotective effects of omega-3 fatty acids, including the reduction in blood pressure, chronic inflammation and platelet aggregation, to at least partially explain why omega-3s are good for the heart. Future treatment studies should define the omega-3 intake (and Omega-3 Index) that optimizes this aspect of cardiac function.”
Dr. James H O’Keefe, MD, a cardiologist and Medical Director of the Charles and Barbara Duboc Cardio Health & Wellness Center at Saint Luke’s Mid America Heart
Institute in Kansas City, MO, and a Professor of Medicine at the University of Missouri-Kansas City (who was not involved with the study) remarked that this research provides “strong data supporting the robust cardiovascular benefits of omega-3 fatty acids.”
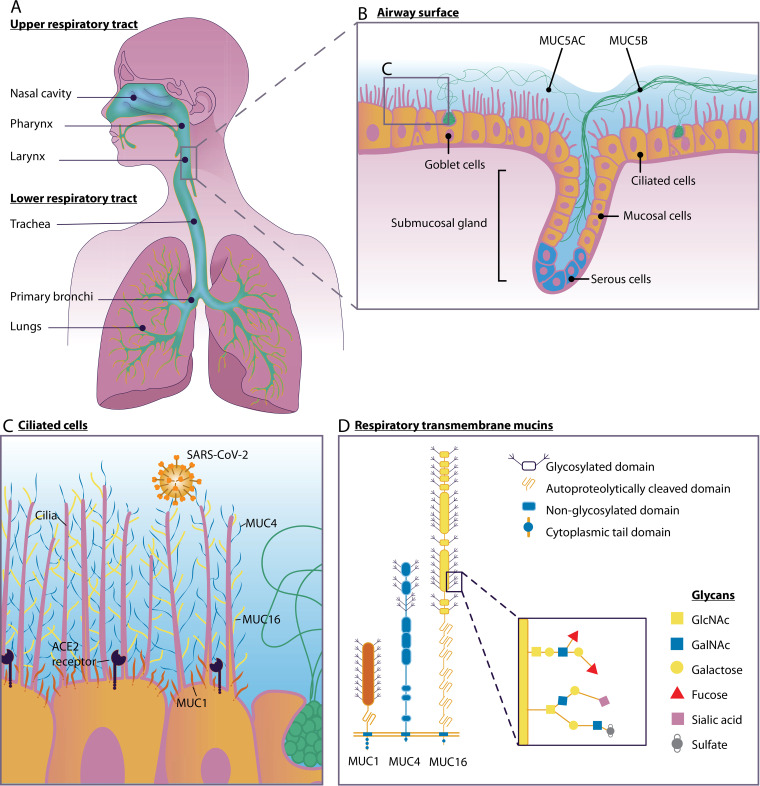
Mucus plays a pivotal role in protecting the respiratory tract against microbial infections. It acts as a primary contact site to entrap microbes and facilitates their removal from the respiratory tract via the coordinated beating of motile cilia. The major components of airway mucus are heavily O-glycosylated mucin glycoproteins, divided into gel-forming mucins and transmembrane mucins. The gel-forming mucins MUC5AC and MUC5B are the primary structural components of airway mucus, and they enable efficient clearance of pathogens by mucociliary clearance. MUC5B is constitutively expressed in the healthy airway, whereas MUC5AC is upregulated in response to inflammatory challenge. MUC1, MUC4, and MUC16 are the three major transmembrane mucins of the respiratory tracts which prevent microbial invasion, can act as releasable decoy receptors, and activate intracellular signal transduction pathways. Pathogens have evolved virulence factors such as adhesins that facilitate interaction with specific mucins and mucin glycans, for example, terminal sialic acids. Mucin expression and glycosylation are dependent on the inflammatory state of the respiratory tract and are directly regulated by proinflammatory cytokines and microbial ligands. Gender and age also impact mucin glycosylation and expression through the female sex hormone estradiol and age-related downregulation of mucin production. Here, we discuss what is currently known about the role of respiratory mucins and their glycans during bacterial and viral infections of the airways and their relevance for the novel coronavirus severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Understanding the impact of microbe-mucin interaction in the respiratory tract could inspire the development of novel therapies to boost mucosal defense and combat respiratory infections.
Mucosal defense in the respiratory tract during SARS-CoV-2 infection. (A) Human upper and lower respiratory tracts. (B) Respiratory epithelium with ciliated cells, goblet cells, and a submucosal gland. The soluble mucin MUC5AC is secreted by goblet cells, and the soluble mucin MUC5B is secreted by mucosal cells in the submucosal gland. (C) Ciliated epithelial cells express transmembrane mucins MUC1 (red), MUC4 (blue), and MUC16 (yellow) and the SARS-CoV-2 entry receptor ACE2. (D) Domain structure of transmembrane mucins MUC1, MUC4, and MUC16. Mucin O-glycan structures and, specifically, terminal sialic acids play an important role in virus-mucin interactions.
(b. Torsaker, Sweden, 30 June 1873; d. Lund, Sweden, 4 December 1952)
Physiology.
The son of Per Erik Thunberg, a merchant, and of Wendela Maria Elisabeth Hård, Thunberg studied medicine at the University of Uppsala from 1891 to 1900 and obtained the M.D. degree with a dissertation on epidermal sensory perception. He was demonstrator for Olof Hammarsten at the Institute of Physiological Chemistry in 1893–1894 and for Frithiof Holmgren at the Institute of Physiology at Uppsala in 1894–1896. He was reader in physiology at Uppsala in 1897–1904. Immediately after the death of Magnus Blix in 1904, Thunberg went to Lund as temporary occupant of the chair of physiology and embryology; the following year he was appointed to the chair of physiology, from which he retired in 1938.
Thunbergs first work, on sensory physiology, was published in 1893 and his last, in 1953. Thunberg extensively studied the physiology of epidermal sensations, showing, among other things, that a pinprick gives rise to two sensations of pain, the second occurring some seconds after the first. This phenomenon was interpreted much later by Zotter-man, who demonstrated the existence of two groups of pain fibers, one of which transmits impulses more slowly than the other. In 1905 Thunberg wrote the chapter “Physiologie der Druck-, Temperatur- und Schmerzempfindungen” for Nagel’s Handhuch der Physiologie des Menschen. With this work he left a field into which he had been led more by chance than by ability.
In 1903, when Thunberg began to study the elementary processes of metabolism–studies that constitute his major contributions to science–nothing was known of the oxidation processes in the tissue cells. Energy is derived in the cells by combustion (cellular respiration), whereby oxygen is consumed and carbon dioxide produced. Lavoisier had proved that respiration is chemically a combustion process in the 1770’s. From then until 1875, the consumption of oxygen and the production of carbon dioxide were thought to be confined to the lungs and the blood. In that year Pflüger proclaimed: “Cells are constantly burning, although we do not see their light with our weak vision.” Everyday experience shows that organic material does not burn in oxygen at body temperature, so it was assumed that oxygen was activated in some way. From about 1840 a series of oxygen activation theories appeared: but valid knowledge had to await the work of Thunberg, Otto Warburg, and Heinrich Wieland. Warburg introduced the term Atmungsferment and argued that this enzyme that catalyzed oxidation was an iron-pyrrole complex. His idea was based on the orthodox concept that the degradation and combustion of food to carbon dioxide and water took place through the direct attack of oxygen on the carbon atoms of the food. Thunberg and Wieland developed an entirely new conception, rivaling that of Warburg.
In 1908 Thunberg began to study the capacity of cells to burn various organic acids, including acetic, propionic, oxalic, malic, succinic, and citric. These acids were not then recognized as normal constituents of the body that played a role in intracellular metabolism; rather, they were known as products of putrefaction or fermentation. From among all the organic acids Thunberg chose precisely those that proved useful to his aims, thus revealing his unerring sense for the right path to follow.
Wieland turned to this area of investigation just when his cooperation was needed to elucidate the nature of the processes of biological oxidation. In 1912 he found that organic compounds can be oxidized through removal of hydrogen in the presence of a catalyst and that the hydrogen can be taken up by suitable acceptors, such as methylene blue. From 1910 Thunberg integrated Wieland’s discoveries with his own, especially those on the biological oxidation of succinate, and initiated the concept of the specific, hydrogen-activating, chain-forming enzyme systems. When Thunberg began this work, all that was known of intracellular enzymes was merely that postmortem autolysis was catalyzed by proteolytic enzymes. Oxidases also had been found.
Thunberg saw that the oxidation of succinate was initiated by an agent in the cells that endowed a hydrogen group in the succinate with a reactivity that it had not previously possessed. The reactivity could easily be demonstrated with methylene blue, which was decolorized by hydrogen uptake. Under the influence of this agent in the cells, the succinate emerged as “hydrogen donator” and released a hydrogen group to the “hydrogen acceptor” methylene blue. The terms “donator” and “acceptor” were introduced by Thunberg and are now in general use. He called the enzymatic agent a dehydrogenase, in this case succinate dehydrogenase. The introduction of the methylene blue method in 1916 opened up a worldwide search for dehydrogenases. The chainlike degradation of the various organic molecules in the organism could now be charted.
Thunberg finally formulated the following generalization concerning the oxidative degradation of food: the degradation is accomplished by a chain of consecutive splittings of hydrogen atoms carried out by a series of dehydrogenases, each with a specific purpose.
With the discovery of a hydrogen-carrying flavo-protein, das gelbe Atmungsferment, Warburg in 1932 contributed substantially to Thunberg’s conception of hydrogen transport from one system to another as a central mechanism in oxidative metabolism. Thunberg rightfully considered himself responsible for a revolution in the concept of the mechanism of biological oxidation.
In 1905, the year of his appointment to the chair of physiology at Lund, Thunberg recorded that nerve tissue respires, taking up oxygen and giving up carbon dioxide. It had previously been thought that nerve fibers conducted impulses like an electric cable, without measurable energy consumption. Thunberg made this discovery with his micro-respirometer, an ingenious device with which he could measure oxygen consumption and carbon dioxide production in small units of tissue. Using this apparatus, he also could demonstrate that traces of certain metals, such as manganese salts, strongly catalyze tissue respiration. This field held his interest throughout his retirement.
Although a scientist first, Thunberg was not unfamiliar with the nonscientific world. As a student at Uppsala he was associated with the radical-liberal group Verdandis, headed by the physiologist Hjalmar Öhrvall. During five decades– through books, popular journals, pamphlets, and the daily press, and as an adviser to the government–he disseminated information on hygiene and medicine that in scope and quality was unparalleled in Sweden.
Thunberg’s enormous capacity for work was combined with good health, and he reached the age of seventy before becoming seriously ill, with pneumonia, from which he recovered. He was fully active for more than nine years, until October 1952, when he stumbled over the doorstep of his house and broke his femur. Despite the best care, he died early in December. He had been elected a member of the Royal Swedish Academy of Sciences in 1928, and later of many foreign learned societies.
BIBLIOGRAPHY
Obituaries include Georg Kahlson, “Thorsten Thunberg.” in Acta physiologica scandinavica, 30 (1953), supp. 1ll: and F. G. Young, “Prof. T. Thunberg,” in Nature (12 Dec. 1953).